Assessment of Learning Disabilities
Assessment of Learning Disabilities:
Cooperation between Teachers, Psychologists and Parents
_____ African edition _____
Edited by Tuija Aro and Timo Ahonen

Cooperation between Teachers, Psychologists and Parents
____ African edition ____
Edited by Tuija Aro and Timo Ahonen
This African edition is based on the original publication by Mika Paananen, Tuija Aro,
Nina Kultti-Lavikainen & Timo Ahonen (2005). Oppimisvaikeuksien arviointi: Psykologin,
vanhempien ja opettajien yhteistyönä. Finland: Niilo Mäki Institute ©
Translation of the original Finnish text: Molehill Communications / Aki Myyrä
Proofreading of the African edition: Kalle Rademacker
Editorial team: Pia Krimark, Niilo Mäki Foundation, Lusaka, Zambia and Susanna Kharroubi,
University of Turku, Finland
Photography: Mr. Mumba E. Mwaba, Timeslice World, Zambia
Layout: Mirja Sarlin, University of Turku, Finland
Printed by: Suomen Yliopistopaino Oy – Uniprint (2011)
This book is published in collaboration with University of Turku, Finland and
Niilo Mäki Institute, Jyväskylä Finland.
1. edition 2011
ISBN: 978-951-29-4687-7 (painettu)
ISBN: 978-951-29-4688-4 (verkko)
Contributors
Ahonen, Timo, PhD
Professor of Developmental Psychology
Department of Psychology
University of Jyväskylä, Finland
Aro, Mikko, PhD
Professor of Special Education
Department of Educational Sciences
University of Jyväskylä, Finland
Aro, Tuija, PhD
Senior researcher
Niilo Mäki Institute Jyväskylä, Finland and
Senior lecturer
Department of Psychology
University of Jyväskylä, Finland
February, Pamela, M.Phil
Senior Lecturer
Department of Educational Psychology and
Inclusive Education
University of Namibia, Namibia
Haihambo, Cynthy Kaliinasho, PhD
Senior Lecturer
Department of Educational Psychology and
Inclusive Education
University of Namibia
Hengari, Job Uazembua, M.Phil
Senior Lecturer
Department of Educational Psychology and
Inclusive Education
University of Namibia, Namibia
Imasiku, Mwiya. L., PhD
Head of Department
Department of Psychology
University of Zambia, Zambia
Kwena, Jacinta, PhD
Senior Lecturer
Department of Educational Psychology
Kenyatta University, Kenya
Matafwali, Beatrice, PhD
Head of Department/Lecturer
Department of Educational Psychology,
Sociology and Special Education
University of Zambia, Zambia
Miyanji, Osman, Dr
Childneurologist/Consultant
Gertrude´s Children Hospital
Nairobi, Kenya
Mkandawire, Lomazala, B.Ed
Senior Lecturer
Department of the Education for the Children
with Learning Disabilities
Zambia Institute of Special Education, Zambia
Muindi, Daniel, PhD
Senior Lecturer
School of Education
Kenyatta University, Kenya
Munsaka, Ecloss, PhD
Lecturer
Department of Educational Psychology,
Sociology and Special Education
University of Zambia, Zambia
Möwes, Andrew Dietrich, PhD
Senior Lecturer
Department of Educational Psychology and
Inclusive Education
University of Namibia, Namibia
Jere-Folotiya, Jacqueline, MA
Lecturer
Department of Psychology
University of Zambia, Zambia
Kachenga, Grace Mulenga, M.Sc.
Principal
Zambia Institute of Special Education, Zambia
Kalima, Kalima, M.Ed
Lecturer
Department of Educational Psychology,
Sociology and Special Education
University of Zambia, Zambia
Kariuki, David, MA
Lecturer
Department of Educational Psychology
Kenyatta University, Kenya
Kasonde-Ngandu, Sophie, PhD
Senior lecturer
Department of Educational Psychology,
Sociology and Special Education
University of Zambia, Zambia
Kharroubi, Susanna, MSc
Project manager
University of Turku, Finland
Koponen, Tuire, PhD
Senior researcher
Niilo Mäki Institute
Jyväskylä, Finland
Kultti-Lavikainen, Nina, Psych. Lic.
Clinical Psychologist
Niilo Mäki Institute
Jyväskylä, Finland
Mwaba, Sydney, PhD
Senior Lecturer
Department of Psychology
University of Zambia, Zambia
Namangala, Phanwell H., MA
Lecturer
Department of Psychology
University of Zambia, Zambia
Ndalamei, Inonge Mwauluka, B.Ed
Senior Lecturer
Department for the Visually Impaired
Zambia Institute of Special Education,
Zambia
Ndambuki, Philomena, PhD
Senior Lecturer
Department of Educational Psychology
Kenyatta University, Kenya
Otieno, Suzanne Adhiambo, MA
Niilo Mäki Institute
Jyväskylä, Finland
Paananen, Mika, Psych. Lic.
Clinical Neurosychologist
Niilo Mäki Institute
Jyväskylä, Finland
Phiri, Gawani Douglas, B.Ed
Senior Lecturer
Department for the Hearing Impaired
Zambia Institute of Special Education,
Zambia
Foreword
Timo Ahonen, Tuija Aro and Susanna Kharroubi
In every class there are probably some children with learning difficulties. Perhaps the child cannot learn to read fluently or may not be able to learn multiplication tables by heart. He or she may be slow at mental calculation or finds learning new motor skills problematic – there are many types of difficulties. During their career, every teacher meets several children for whom learning is laborious and even children who think that they cannot learn. Teaching these children is a challenge for the instructor. In fact, it is a challenge for the entire school. This book was written for teachers, educational or school psychologists and parents to guide them in helping children to overcome the challenges of learning difficulties.
Education for the Children with Learning Disabilities: African-European Co-operation for Promoting Higher Education and Research project was a joint action between Psykonet – University Network in Psychology from Finland coordinated by the University of Turku; University of Namibia Department of Educational Psychology and Special Education; University of Zambia Department of Psychology; University of Zambia Department of Educational Psychology, Sociology and Special Education; Zambia Institute of Special Education; Kenyatta University Department of Educational Psychology; and Niilo Mäki Institute (Finland). The project aimed at enhancing the curricula of the African partner institutions in the field of learning disabilities among school children.
This book is an outcome of three years of systematic and successful work between the project partners. This publication which is considered a “training standard” forms together with the Guidelines on Learning Disabilities and the Instructions for Local Authorities (published in 2011 in the newsletter Learning and Learning Disabilities in Africa) an integral part of the partner institutions´ curricula on learning disabilities.
The book was written by a multiprofessional and multicultural group of experts on learning disabilities, and it combines the best practices from Finland, Kenya, Namibia and Zambia. The concept of learning disabilities is relatively new in Africa although the phenomenon of children with learning difficulties or those described as “slow learners” is not (Abosi, O. 2007). There is no particular definition of learning disability that one can refer to as “the African definition”. The term refers to children who experience learning difficulties independent of obvious physical defects such as sensory disorders. It is understood that children with learning difficulties have the ability to learn but that it takes them a longer time to comprehend things than the average child (Abosi, O. 2007). Also, African experts base their concept of learning disabilities on Western definitions such as follows:
Learning disability – is a general term that refers to a heterogeneous group of disorders manifested by significant difficulty in the acquisition and use of listening, speaking, reading, writing, reasoning, or mathematical abilities. These disorders are intrinsic to the individual, presumed to be due to central nervous system dysfunction, and may occur across the life span. Problems of self-regulatory behaviour, social perception and social interaction may exist with learning disabilities, but do not by themselves constitute a learning disability. Although learning disabilities may occur concomitantly with other handicapping conditions (for example sensory impairment, mental retardation, social and emotional disturbance) or with extrinsic influences (such as cultural differences, insufficient or inappropriate instruction), they are not the results of these conditions or influences (National Joint Committee on Learning Disabilities, NJCLD, 1988, 1993).
Similarly Hammill (1990) has put the concept of learning disability (LD) into a nutshell as follows:
LD is marked by heterogeneity, LD is probably the result of CNS dysfunction, LD involves psychological process disorders, LD is associated with underachievement, LD can be manifested in spoken language, academic or thinking disorders, LD occurs across the life span, and LD does not result from other conditions.
When problems with learning are first observed, an attempt is made to uncover their causes and source, which are often uncertain. In Finland, parents and teachers can usually obtain help from the school psychologist in uncovering the causes of problems, as well as from health and social services personnel. There are established practices and evaluation methods for assessing learning difficulties. How the information gathered with various methods can be utilised to promote the child’s learning is a challenge for the teachers, school psychologist, and also the health and social service workers. In African countries, the evolution of school psychology services closely follows a developmental pattern: First priority is given to the widespread provision of general education services that precede the special education services and school or educational psychology services. This means that many countries of sub-Saharan Africa are still lacking these services, especially in rural areas, despite communities, schools, and students having needs that can be met by school psychology services. These needs include educational support (the focus of this book) as well as stress and health management in view of the pressures on children and their families due to industrialisation, poverty and disease (Mpofu, Peltzer, Shumba, Serpell, & Mogaji, 2005).
The first part of this book briefly describes what efficient learning requires from the school, class, family and child. “Learning disability” is defined and a line is drawn between learning disabilities and school difficulties resulting from other causes such as inadequate school management, lack of well-trained and effective teachers in the schools, large class sizes, providing early primary education in an international language that is not the child’s mother tongue, lack of teaching materials, and unfortunately – still – sometimes negative attitudes among some teachers toward children with disabilities and their inclusion in regular schools as a result of teachers’ traditions and culture, as described by Abosi (2007).
The second part presents a four-step assessment model for learning disabilities, which emphasises cooperation between the school, the family, and the school or educational psychologist. The third part of the book describes difficulties in academic skills and cognitive functions, and their assessment. The development and sub-processes of each skill and function are described in detail to facilitate assessment. We are painfully aware that there is still a huge amount of work to do in developing adequate and culturally acceptable assessment tools for teachers and psychologists in African countries working with children who have learning disabilities (see Grigorenko, 2009) We really hope that this book will stimulate these efforts. The final part summarises the theoretical discussion of the earlier parts of the book and introduces the interpretation of assessment results. It also shows how conclusions can be made based on the results, and how support can be planned for the school, class and home.
The book is meant for teachers, special education teachers, and psychologists who perform learning disability assessments, as well as for therapists in various fields. It offers basic information about learning disability assessment, the relationship between academic skills and cognitive functions and the development of these skills, as well as the significance of their development for learning.
We wish to thank numerous professionals who have contributed to this book with their valuable comments in Finland, Kenya, Namibia and Zambia. Our special gratitude goes to the University of Turku for coordinating the project, and the University of Jyväskylä and the Niilo Mäki Foundation for their active role in the project planning an implementation.
References
Abosi, O. (2007). Educating children with learning disabilities in Africa. Learning Disabilities
Research & Practice, 22, 196–201.
Grigorenko, E.L. (Ed.)(2009). Multicultural Psychoeducational Assessment. New York: Springer
Publishing Company.
Hammill, D.D. (1990). On Defining Learning Disabilities: An Emerging Consensus. Journal of
Learning Disabilities, 23, 74–84.
Mpofu, E., Peltzer, K., Shumba, A., Serpell, R., & Mogaji, A. (2005). School psychology in
sub-Saharan Africa: results and implications of a six-country survey. In C.L. Frisby & C.R.
Reynolds (Eds.), Multicultural School Psychology (pp. 1128–1150). Hoboken NJ: John
Wiley & Sons.
Tuija Aro, Jacqueline Jere-Folotiya, Job Hengari, David Kariuki and
Lomazala Mkandawire
1. Learning and learning disabilities
What factors at school and in educational environments affect a child’s learning?
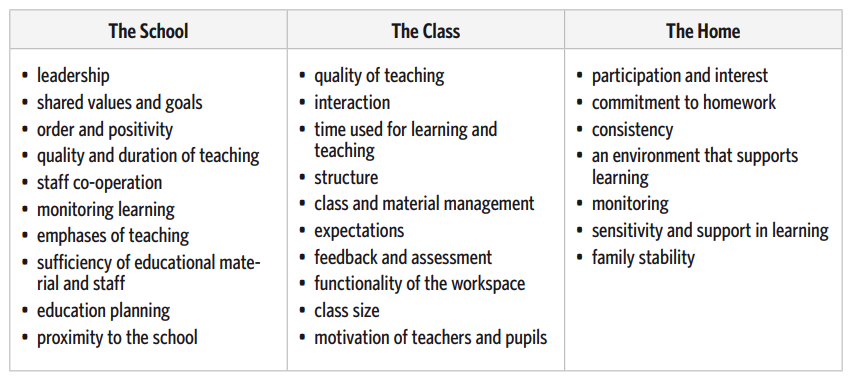
School learning is affected by many factors. The personal characteristics of the child, familial attributes, and factors related to the school and class altogether affect the child’s ability and potential to benefit from teaching. These factors influence the child’s learning experiences and in the process affect the child’s self-image as a learner, among many other attributes. These experiences, the child’s beliefs, and his/her knowledge and skills, together with the characteristics of the environment, form a complex interactional system. Understanding this system helps us to understand the underlying factors in children’s learning difficulties which is a prerequisite for planning and implementing effective pedagogical and intervention strategies. Scientific research on school learning has examined various school factors, which include school systems, and schools’ organisational structures and curricula (see e.g., Wang et al., 1994). Some of this research has focused on factors pertaining more directly to the child, such as the child’s characteristics and the teaching methods used in the school. These studies reveal that child-related factors, as well as family and close community-related factors, are central to the effectiveness of learning. However, we must not focus merely on the child and his/ her skills or lack of skills as we examine problems with learning. We must perceive the child as a part of his/her environment, understanding that today’s difficulties may spring from the child’s early experiences and familial factors in addition to the impact of diverse environmental variables, cultural customs, and other unique local structures. All these factors are discussed in detail in the following sections.
Table 1. Factors within the child’s various environments that affect learning (following Christenon &
Ysseldyke, 1989; Reynolds, 1997)
Box 1. Finland – An example of a success story in basic education
Based on different international comparative studies, we know that the Finnish school system has been
very successful:
- The IEA Study in 1991 (International Association for the Evaluation of Educational Achievement): Finnish student , aged 9 and 14 years, were found to be the best readers in the Reading Literacy category
- The IALS in 1998 (International Adult Literacy Survey): Finnish young adults, aged 16 to 25 years, also outperformed their peers in other countries.
The same conclusions have been drawn by the PISA (Programme for International Student Assessment) studies in 2000, 2003 and 2006. More specifically, in 2000, a total of 265,000 fifteen-year-old students from 32 countries took part in the PISA study. The PISA assessed literacy in three domains: Reading, Mathematics and Science. The PISA assessed particularly young people’s capacity to use their knowledge and skills in order to meet real-life challenges, rather than merely looking at how well they had mastered a specific school curriculum. Reading literacy is a key competence in today’s society because it contributes to an individual’s mental growth, learning, work and active citizenship. Reading literacy is based on basic technical reading as well as on a broader conception of reading where stress is laid on the construction of meaning from the text. It is very interesting that the average literacy level of a nation’s population is an even better predictor of economic growth than its overall educational level. The PISA studies show that the Finnish educational system has succeeded not only academically, but also in promoting relatively high equality among 15–year-olds. Finnish students showed the highest achievement (in 2006 the second highest) in reading literacy. The number of poor readers has been remarkably low in Finland, and the gap between low and high achievements relatively narrow.
Factors behind the high Finnish educational scores in the PISA
- Finnish boys are good readers, but Finnish girls are even much better than Finnish boys.
- Even the lowest-performing Finnish schools are very good compared to the OECD’s average, possibly due to more equal opportunities for learning.
- Finland’s lowest-scoring students perform better than their comparative students in other OECD countries (including in mathematical and scientific literacy).
- The difference between top performers was much less pronounced.
- The positive effect of the Finnish strategy of supporting students from disadvantaged back grounds and with learning disabilities could be seen in the results of the PISA studies in 2000, 2003 and 2006. The impact of parent’s socioeconomic status on students’ performance was relatively low.
- Finnish students’ engagement in reading is very high, especially among the girls positive attitudes toward reading, frequency of reading diversity of reading material.
General background of Finland’s educational success
- The high quality and comparatively high equality of basic education is grounded in a publicly funded system of education that is comprehensive and non-selective.
- Schools are open to all children, irrespective of their gender, place of residence, language, or socioeconomic background.
- The effort to minimise low achievement and boost inclusion has proved successful. Minimal between-school variation is one of the key factors associated with high performance.
- There is no connection between a school’s status and the average performance of its students. It seems to make little difference, where a student lives or which school he or she attends – opportunities to learn are the same, but male gender and immigrant background seem to increase the risk of low-achievement also in Finland.
- Pedagogical philosophy and practice: The school is there for every child and the school must adjust to the needs of each child, not the other way around.
- Reasonable class size (on average 19 students per class in grade 9, in 2003) and support, as well as part-time special education (received on average by 20 % of students during their nine years of schooling) for children with learning disabilities are offered.
- Student welfare groups are active in the schools (consisting of teachers, principals, counsellors, psychologists, school nurses and doctors).
- Well-educated teachers abound since all teachers, even those teaching primary grades, have a master’s degree (MA) either in Educational Science or, if different, in their respective field of teaching. Teachers also have considerable pedagogical autonomy in the classroom in respect to organising their work within the flexible limits of the national curriculum’s framework.
Conclusion
There is no single secret or key behind the success of the Finnish educational system. High performance is related to cultural factors, the educational system, curriculum, pedagogical and assessment practices, and to individual characteristics of the students and their families.
Read more:
Linnankylä, P. & Arffman, I (Eds.) (2007). Finnish Reading Literacy. When quality and equity meet. University of Jyväskylä: Institute for Educational Research.
The school as a factor
In all communities, the school is considered as an important decision maker and implementer of teaching and support for learning. An effective teacher is one who is proficient in planning and implementing teaching programmes in addition to making sound decisions regarding remedial strategies geared towards catering for individual differences among learners. In many African countries, the curriculums are rather rigid and the teachers are compelled to follow the syllabus that has been laid down. In the African context, as in Zambia, Namibia and Kenya, the schools follow a basic curriculum formulated by the respective Ministries of Education. For each grade level, a syllabus is available based on the curriculum, and from that syllabus teachers are expected to formulate their teaching plans using the teaching schemes as well as the teachers’ guides and pupils’ text books. In Finland, teachers have more freedom to plan their teaching. This trust in teachers’ professional competence is based on the high quality of the teacher training at the master’s degree (MA) level.
The support that the child and his/her family receives from the school, as well as the cooperation between the home and the school, is essential for the assessment of learning disabilities and the implementation of intervention strategies. Cooperation among students, parents, the school and the community in general is vital for the well-being of the student. Moreover, the support of the heads of school for the teacher helps both parties to develop good practices and inspires a belief in the significance of their respective roles at the school and its organisation. Accordingly, advice and instructions from such key figures can be helpful in teachers’ daily work, particularly in the development of explicit decisions relating to work and teaching.
Research results from a survey conducted by the Southern African Consortium for Monitoring Educational Quality (SACMEQ) on the conditions of schooling and the quality of primary education has demonstrated that little success has been achieved in improving the quality of education, particularly at the primary level. This survey included several countries, amongst them Zanzibar, Namibia, Lesotho, Botswana, Zambia, Malawi, Mozambique, and South Africa. The SACMEQ (2004) report pointed out that the academic results at the primary level are very poor. The report states that, at the national level in Namibia, in 1995, only 22.7 % of learners reached the minimum level of mastery (i.e., likely to barely progress to the next grade) in reading literacy and a meager 7.8 % reached the desirable level of mastery (i.e., high likelihood of progressing to the next grade). In comparison, the figures for the year 2000 show a decline in the percentages of learners at the minimum and desirable levels of achievement, with 16.9 % of learners having a minimum level of mastery and only 6.7 % of learners having the desirable level of mastery. These results show a worrisome situation, indicating that the commendable expansion of the provision of access to primary education has not been accompanied by a corresponding improvement in the quality of learning outcomes. In Namibia, this was attributed partly to the lack of a comprehensive Early Childhood Development programme, and pre-primary education interventions are needed for better educational outcomes. Accordingly, the ETSIP (2007) programme identified early childhood development and pre-primary education as playing a central role in the overall development of children and their chances of future success in school.
The classroom as a factor
According to research, the class experiences and teaching have a greater effect on learning results than the general policies and operations of the school (see Wang et al., 1994), highlighting factors like the feeling of affinity for the class, reward structures, goal orientation and workable routines. When the classroom is examined as a workplace, factors like the functionality of the room and furniture, an appropriate interior design for teaching, sufficient lighting, and a peaceful workplace ambience collectively rise to importance.
Students generally respond well when the teacher uses various sensory modalities during teaching. In lower grades, students enjoy the use of a combination of visual and tactile cues in addition to the use of intrinsic motivators. Also significant for learning is how much time students take to perform given tasks and how often they perform tasks in which they can succeed. In addition, attention must be paid to the way homework is inspected and to the feedback students receive from the teacher and each other. These actions affect, for example, the meanings that children assign to tasks and the work they perform, and help to guide children’s attention towards matters essential for success.
From the viewpoint of classroom functionality, the teacher’s skills in managing and guiding the class are vital. This includes efficient daily practices and the use of teaching materials, as well as controlling disturbing factors and problem behaviour within the class. The amount and quality of interaction in learning and teacher-student relations also affect the efficiency of learning. Interaction in learning includes, for example, feedback from the teacher, various questions asked by the teacher and instructions concerning knowledge enrichment, all of which affect the development of the child’s information structures. Furthermore, social interaction outside of teaching situations is particularly important for the development of the child’s self-esteem and feelings of affinity, which are known to affect learning results as well.
The content and quality of teaching can be assessed, for example, by examining the way that the teaching content is presented and considering the practices used to instruct students. For example, in Zambia the Primary Reading Programme (PRP) was introduced to help improve reading and writing skills for children in all Government schools from grade 1 to grade 7. Under this programme, the teaching of initial literacy is conducted using the New Breathrough to Literacy (NBTL) course in grade 1. In this course initial literacy is taught in each of the seven official Zambian languages, each language catering for a specific region of the country. In grade 2, the Step Into English (SITE) course is used. This course enables the transfer of the literacy skills from the Zambian languages to English. From grade 3 to 7, the Read On Course (ROC) consolidates what was taught in grades 1 and 2 in both English and the Zambian languages.
The various syllabi used in the basically aid the teachers in the preparation, organisation and presentation of the daily lessons by providing guidance in terms of subject content and how this content can be effectively presented in line with a particular grade level. The content material is designed based on the overall learning objectives and desired outcomes for the children, as stipulated by the Ministry of Education. This is not to say that the teachers themselves have no say in what and how they plan their daily lessons. It just means that they are expected to impart the pupils with specific knowledge as indicated in the syllabus, yet in conjunction with this the teachers are generally expected to use their own initiative and innovation to ensure that the material is presented in a manner that will ensure that their pupils grasp the relevant concepts and skills. In the process of preparing daily lessons, most teachers need to take a number of factors into consideration, such as the class size, the pupils’ current level of knowledge, availability of teaching and learning resources, available time and the general progress of the class, to mention but a few.
The lack of adequate teaching and learning resources is a problem that is faced by many African countries. The lack of teachers in some schools, especially rural schools, affects the learning and teaching process in more general. The number of students is quite high in most classes, with an average of about 50–60 students per class, depending on the location of the school. For example, in Kenya and Zambia, primary education is free of charge, which enables even children from poor homes to receive an education. Due to a lack of resources, this initiative has led to an average of 150 students per class in some public schools in Kenya, in both urban and rural areas. School resources are therefore stretched. The more students there are in a classroom, the more resources are required. Unfortunately, adequate teaching and learning resources, such as sufficient furniture, books and classrooms, are not always available, hindering the learning and teaching process. It must be mentioned, however, that the respective governments are trying by all means to ensure that everything that is needed for children to learn is available.
World Bank studies (Marope, 2005) have pointed out serious lapses with regard to literacy levels and language learning in African countries. The study (Marope, 2005) found that the shortage of textbooks and instructional materials persists especially in primary schools. Other than textbook shortage, schools are characterised by inadequate instructional materials such as student workbooks, teaching aids and enrichment materials. At the end of a school year, learners progressing to the next grade often do not pass their materials from the previous grade on to the new learners even though print materials for reading are rare both in schools and homes. The study also found practicing teachers to have poor reading and grammar skills, weak elicitation techniques, limited vocabulary, as well as limited facility to adequately explain concepts. Marope (2005) argued that teachers’ poor English proficiency in African schools adversely affects instruction, not only in English as a subject, but also in all other subjects that are taught in English. This is crucial in school systems such as that of Namibia, for example, which uses the English language as a medium of instruction from grade 4 onward. Similar to Marope (2005), Sinalumbu (2002) concluded that factors contributing to poor literacy attainment in Namibia include overcrowded classrooms, poor teaching, primary language interference, and lack of parental support in learning to read and write. Also concerning Namibia, as an example of African schools using the English language for classroom instruction, Kuutondokwa (2003) documented the lack of reading materials in schools and homes, illiterate parents, lack of assistance from teachers, improper motivation to read, lack of printed materials in local languages, automatic promotion, poor teaching and poor teacher training programmes, as aspects that warrant attention if the nation is to improve its literacy development and children’s rate of school attendance.
The culture and language of instruction as factors
The issue of several languages being spoken in most of the African counties is essential in respect to school instruction. For example, Namibia has 13 languages of instruction for grades 1 – 3. The writing of some of these languages is still evolving. Standardisation of orthographies and the production of learning materials are recent phenomena that teachers are still getting accustomed to. Because of teachers’ language limitations, reading and writing lessons tend to be imparted with a rather mechanical-sounding verbalisation of words without grasping meaning or context, and likewise copied by the children in the classroom. Given their own challenges, teachers have little facility to identify, assess and intervene in pupils’ learning problems in order to help them with their reading and writing difficulties.
Transitional bilingual education is a common type of educational system, such as in Namibia. Initial literacy learning in the mother tongue is crucial to establishing a positive self-image, an affirmation of one’s own culture, and a greater understanding of the world us. For instance, in Namibia, language skills and literacy tend to first be developed in the mother tongue, until a learner is thought to be proficient enough in his/her mother tongue to cope in mainstream education. It is recognised that children learn best when they are taught in their own mother tongue. After being confident and well-equipped in their mother tongue, mastery of another language under optimal circumstances is considered not to be a problem – a view that is held by several theorists as we shall see. The primary concern in using the mother tongue in instruction is the ability to ensure that all learners acquire the skills which will lay a strong foundation for literacy, communication, and concept formation in numeracy, all of which are crucial in regard to the learner’s future education (see Namibian Ministry of Education, Lower Primary Phase Syllabus, First Language, 2005). The aim of the transition, as argued by Baker (2003), is to gradually increase the use of English in the classroom while proportionately decreasing the use of the mother tongue language in the classroom. This policy of transitional bilingual education promotes the early exit from mother tongue instruction to English instruction. For this to succeed, the teachers at these levels need to be bilingual in order to promote the transition from home language to school language, which is not always the case.
The home as a factor
The significance of the home for efficient learning has always evoked discussion. The family’s primary duty is to offer the child care and nurturing, but the family is also important for the child’s studies. At their best, the family’s actions and attitudes support learning. An appreciative and supportive attitude toward studying is seen, for example, when parents show interest in their child’s school and participate in school events. They supervise their children’s homework and they have expectations concerning school success. When a child is confronted by problems in learning, the parents’ most important task is to offer appreciation and security. In these situations, cooperation with various parties, and sometimes even fighting for the child’s rights, is called for from the parents.
In African countries, many parents also have problems in their own education which might influence the child’s motivation. Research by Gachathi (1976) indicates that there is a high positive correlation between the level of parents’ education and their children’s achievement motivation. Furthermore, Mbenzi (1997) argued that socioeconomic background plays a role in learning to read. He argued that many parents were illiterate and could not render assistance in literacy learning. Poverty has also been pointed out as a stumbling block as disadvantaged parents cannot afford to buy books to share with their children, while affluent parents can purchase the necessary materials for learning. Also, in 2004, in research by the SACMEQ, it was reported that the reading competence of learners from low socioeconomic groups was much lower than that of learners from high socioeconomic groups. In 1995, only 11.1 % of learners at a low socioeconomic level reached the minimum level of mastery, while 34.1 % of learners at the high socioeconomic level reached the minimum level of mastery. The desirable level of mastery for the same year was 1.2 % and 14.2 %, respectively. In the year 2000, only 5.9 % of learners at a low socioeconomic level reached the minimum level of mastery, while 31.9 % of learners at the high socioeconomic level reached the minimum level of mastery. The desirable level of mastery for the same year was 0.8 % and 14.9 %, respectively.
Many African parents, like many other parents around the world, value education for their children. There are different forms of education, but the most prestigious is the formal type of education obtained through academic studies. Not only is it viewed as a source of status for both the family and the individual, but it is also viewed as a means to a better life by the whole community. That is why many African parents make huge material sacrifices to ensure that their children have everything they need to go to school and succeed, saving money for school fees, uniforms, stationary, books, and transport to school among other needs. While there are some parents who may be able to assist their children with school related activities, such as helping with homework or reading with their children, there also exists a large number of parents who are unable to provide this kind of assistance because of their own lack of education. Their lack of education may mean that they are unable to assist with academically oriented activities at home, but it does not take away the hope, desire and motivation to see their children succeed and achieve more than they have as parents. This motivation, enthusiasm, encouragement, faith and hope (all necessary for success) for a brighter future is what they impart to their children.
What does efficient learning require from the student?
The foundation of learning is the child’s inherent curiosity and desire to learn and control himself/ herself and his/her environment. The child is naturally motivated to learn new things and to meet new challenges. Motivation is maintained, for instance, by experiences of success and the joy of mastering new skills. Sometimes this joy and enthusiasm receive such strong blows that the child’s faith in his/her own abilities is weakened and the child subsequently loses the courage to tackle new tasks. Recurring failure may weaken the child’s self-concept as a learner and member of the classroom community to the extent that learning loses its appeal and the child does not learn according to his/her potential. In addition, the child’s courage to face challenges and his/her ability to take initiative in problem-solving situations, as well as to engage in teaching and classroom activities, is diminished. In such a situation, the child needs substantial and prolonged support from his/her peers, significant adults and from the community in general in order to regain faith in his/her ability to learn new knowledge and skills.
Along with age and experiences at school, the child learns to improve his/her working skills. A positive self-concept and metacognitive knowledge and skills that are acquired alongside the skills learned at school and through experience, help the child to develop study practices that are most suitable for him- or herself. These skills are also highly significant for the child’s ability to benefit from teaching and the use of educational materials in his/her coming school years. Research on study-efficacy has revealed the particular importance of metacognitive knowledge and skills, which are essential since they have an impact on the child’s ability to be successful in learning situations and school activities, as well as influencing the ability to apply and generalise what they have learned and to monitor and evaluate their work as an individual and in the group. Children themselves are seldom aware of the strategies they use, which is why adults should pay attention to their child’s lack of strategies for studying or their ineffectiveness. If the child has poor work and study skills, then he/she cannot set goals for him- or herself, nor for studying – this makes it difficult for a child to begin work and to carry it through to completion. The child’s attention may also be diverted by irrelevant issues, or he/she may get stuck on a counterproductive way of carrying out a task – such a child is often dependent on the presence of an adult or on repeated guidance.
Figure 1. The cognitive and emotional prerequisites for effective learning (modified from Meltzer, 1996).
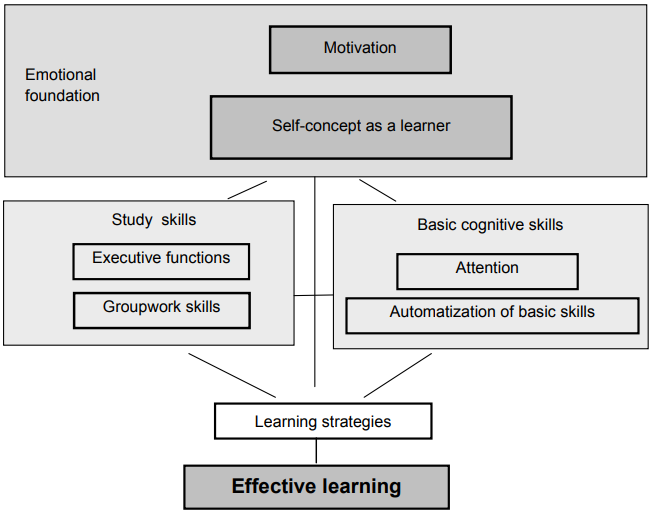
Strong motivation, a positive self-image, and proper study practices and strategies are prerequisites for effective learning. All of the factors which contribute to ineffective learning, as described, are presented in Figure 1. Sometimes these sustain substantial deficits that can hinder learning significantly. Furthermore, properly directed motivation, a positive self-image and effective learning strategies are not always enough to ensure fluent and easy learning of skills. The ability of some children to learn new skills is notably weaker than that of their peers. They need frequent repetition and more practice, or perhaps different teaching methods, in order to learn new skills and to use them as tools for further learning. A child may also have insufficient skills in focusing and sustaining his/her attention. In such a case, a developmental problem that hinders the assimilation of basic skills is responsible for the difficulties in learning. The term “learning disabilities” is usually used with these children.
To understand difficulties in a child’s learning, we must assess several factors that affect learning. By assessing the tasks and situations that cause difficulties, we can clarify what is necessary for the child to succeed in those tasks and situations. Assessing the development of the child’s cognitive skills and emotional development helps to understand his/her strengths and weaknesses. Assessing the learning environment, for its part, tells us how the combination of the child’s characteristics and the demands of the task and situation affect learning, as well as revealing what kind of support and challenges the child is experiencing. The goal of learning disability assessment is to produce knowledge of these different factors affecting children’s learning and to understand how these factors are interrelated.
In learning disability assessment, information is synthesised with the child’s developmental history, the phenotypes of the problems and the environmental factors. Light is also shed on their interaction. Successful learning disability assessment and support planning require the close cooperation of the adults involved in the child’s education. Among other factors, it helps those working with the child to understand the following obstacles in learning:
- Poor motivation or negative self-image as a learner: What has caused their negative development?
- Difficulties in learning basic skills: What kinds of developmental problems are behind these difficulties?
- Lack of learning strategies: What has hindered the learning of effective strategies?
- How do these difficulties interact?
In order to provide answers to these questions we must evaluate a whole series of developmental factors and educational activities, all of which involve the learner, the parent and the teacher.
What are learning difficulties or disabilities?
A learning disability is seen on a functional and behavioural level, in the slow or abnormal learning of new skills. Among school-aged children, difficulties may be seen as deficient skills in
• reading,
• spelling and writing,
• reading comprehension,
• mathematics,
• problem-solving, and
• attention.
According to the diagnostic definition, learning disabilities are thought to be developmental disorders or differences (most often based on genetic factors affecting the development of the nervous system already before birth) that are not due to mental disabilities, neurological disorders or illnesses. A significant criterion, according to the definition, is that deficits in cognitive functions prevent achieving the learning objectives of the age group in spite of sufficient schooling and teaching. The student should receive sufficient teaching, which means special education for the slower learner. But we have to remember that learning difficulties also appear in connection with diagnosed neurological injuries or illnesses (such as epilepsy or traumatic brain injuries), and their scope depends on the location and extent of the injury or the nature of the illness. Neurological injuries and illnesses can also extensively delay the general development of the child. It is thought that in developed countries, with well-developed health care systems and services, the aetiology of learning difficulties is most often genetic. However, the situation may be much different in less developed countries, such as the African nations, where considerable problems in health care systems increase the neurological risks affecting children. Additionally, sufficient teaching is not guaranteed in African countries, chiefly due to inadequate resources to cater for both the gifted and challenged children.
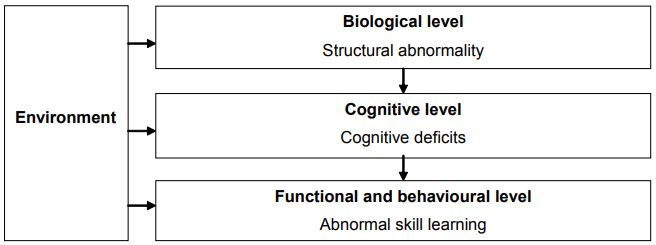
In general, deficits in cognitive functions are believed to be behind learning disabilities. The cognitive characteristics typical for each learning disability are examined in detail in later chapters. An abnormal or atypical organisation of cerebral functions – the causes of which are not yet fully understood – is thought to be behind cognitive deficits. It is commonly believed that an abnormal development of the nervous system results from the overlapping of many different factors of which biological factors, such as heredity, form a significant portion (see Figure 2). Pre-, peri-, and postnatal events may also be significant. This complex relationship between hereditary and environmental factors can be represented as follows:
Development = f(H x E x T), where
f stands for the “function of”
H refers to heredity, i.e., our inherited traits
E stands for the effects of environmental agents which include familial experiences as well
as school and health factors etc.
T is for the passage of time
The above relationship indicates that the three variables (H, E and T) play an interactive role
in influencing an individual’s quality of development.
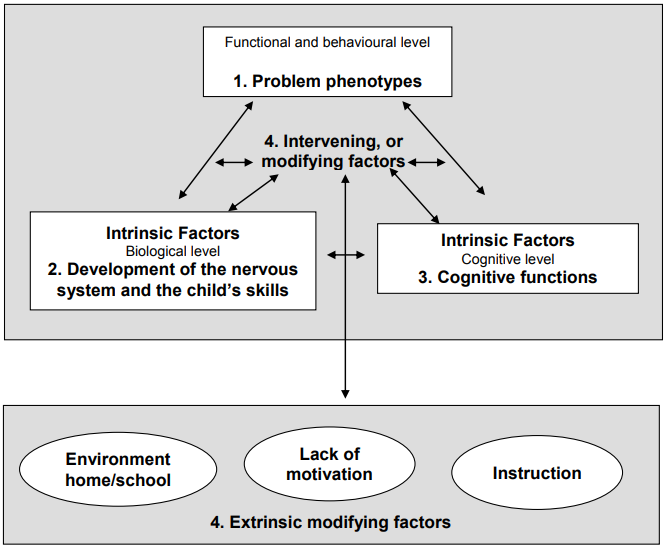
Figure 2. A three-level explanatory model of learning disabilities (Frith, 2001).
A rough distinction can be made between developmental problems detected before schoolage which become manifest as learning disabilities during school-age, and learning disabilities that emerge at the onset of school or later. Developmental problems manifest themselves as problems in the development of attention, language, visual-spatial perception, motor or social skills, or as combinations of these problems. In many cases, such problems manifest themselves before the child reaches school-age, meaning a diagnosis can be made even before the child attends school.
Learning disabilities that arise during the school years are generally difficulties in learning the basic skills taught at school. Most common are learning disabilities in reading, spelling/writing, and mathematics. The aforementioned developmental problems are often behind these difficulties as well, but often the developmental problems (e.g., problems in language development or mild motor difficulties) have been moderate or undetected prior to the child reaching school-age, or they have been diagnosed as insignificant, resulting in the child not receiving any special support. In Finland, it is a common procedure in the examination of five-year-olds at the child health clinic to make a more detailed assessment of the child’s development than on earlier visits. This offers an opportunity to detect any possible delays or deficiencies in development and to commence with relevant support for the child before school begins. Also in Kenya and other African countries, possibilities for early identification do exist due to the rapid enhancement of services for the children with special needs there; however, a lot of children have not yet received these very essential services.
What other factors may impair learning?
Learning disabilities are not the only cause for difficulties in learning. It is often hard to distinguish a learning disability from a learning difficulty caused by something else, or to draw distinct boundaries for when a child has a learning disability and what the cognitive deficit is that predisposes them to the disability. A defining issue in so-called specific learning disabilities has traditionally been the difference between the child’s general intellectual capabilities and his/her specific learning results. According to this thinking, developmental difficulties and learning disabilities appear as a slower development in some specific skill area.
However, the notion that learning disabilities can also be detected in those children and adolescents who have wide-ranging cognitive deficits is gaining ground. According to this school of thought, for instance, the cause behind reading disabilities is a difficulty in processing phonological information, which impairs learning to read regardless of the person’s general performance level. Additionally, a familiar phenomenon in practical work is the so-called Matthew Effect, in which difficulties in one function gradually expand their effect to other areas as well. For example, the consequences of deficient reading skills can be seen in poor performance even in tasks that do not demand reading. Infrequent reading results in, for example, meagre accumulation of general knowledge and vocabulary, low self-esteem and motivation, and poor general performance in both school and test situations. Thus, the modern understanding of the relationship between learning disabilities and general aptitude is not as unambiguous as it is in some of the more traditional definitions of learning disabilities.
Biological risks (such as chromosomal and genetic anomalies) do not directly define the phenotype of learning disabilities. Various factors pertaining to the child’s environment, social relations, interaction and motivation determine the forming of reciprocal relationships between nervous system development, abilities, skills, performance and behaviour. We can also assume that there are children without serious risk factors affecting their cognitive skills or nervous system development, but whose disposition towards learning disabilities is realised in unfavourable circumstances. Factors in the child’s environment can amplify or highlight problems with learning. Respectively, an environment that supports the child’s development may deter learning disabilities or prevent their deepening or expansion. For example, it has been observed that the impact of early developmental risk factors on a child’s development is also connected with his/her growing environment and the support that the child and his/her family receive, rather than only with the original biological risk. While studying a child’s learning skills and knowledge, one should assess whether there are factors in the child’s life that obstruct or hinder his/her learning and school attendance. Such factors may be, for example:
- teaching and school-related problems (e.g., number of pupils in the class, education of
- the teacher, teaching materials and books),
- insufficient nutrition or sleep,
- health problems,
- problems in the child’s emotional development and security,
- the effect of a family member’s emotional problems (e.g., anxiety or depression) on the child,
- violence in the family,
- social/economical problems of the family, and
- ambiguous daily routines at home or school, insufficient support.
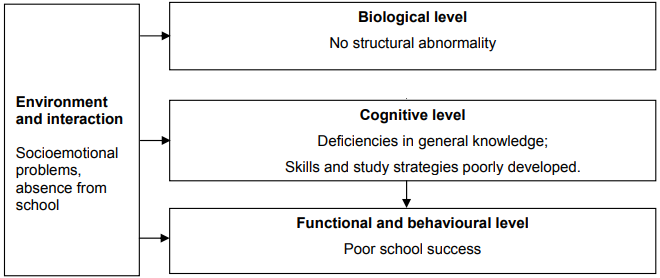
Problems in learning due to the aforementioned factors, may manifest themselves in daily situations of difficulties with schoolwork, similarly as with learning disabilities (see Figure 3). A picture of the child’s daily life and family’s situation can be formed by carefully gathering developmental information and evaluating the school and family situation. Sometimes it can be noted that risks in the child’s environment coincide with cognitive-based learning disabilities. In such a case, it is important to form as comprehensive a picture as possible of the factors affecting the child’s learning, for the sake of successful support planning. In Africa, schools are considered to be the society’s property, which is why school boards have a very strong representation of parents. Teachers are held accountable for pupils’ performance, sometimes to unrealistic levels – especially regarding the children with learning difficulties (Ondiek, 1986).
The assessment of learning disabilities and the discernment of these from learning difficulties caused by external factors is even more challenging in African countries than in Finland. This is readily seen in the results of Nepando (2003), who concluded that poor preschool services, poor teacher training and preparation, poor learner motivation, reading anxiety resulting from labelling, grouping, humiliations and unfair treatment of poor readers and writers resulting in emotional block, lack of support services to help teachers and parents with children who find it difficult to master literacy skills, overcrowded classrooms with no room for individual attention, and insufficient teaching and learning materials, are all affecting literacy development amongst African children.
Figure 3. Problems in school attendance due to socioemotional factors (according to Frith, 2001; cf.,
Figure 2).
Knowledge of the child’s general situation in life and the typical characteristics of learning disabilities can be used to support evaluation. Firstly, learning disabilities do not usually appear suddenly or as a regression or loss of skills. Usually, slower development of specific skills has been apparent during the child’s growth, or the child has achieved certain developmental steps a little bit later than is typical for his/her age group. The basic skills taught at school can also be seen as developmental steps. For example, learning to read is normally a developmental and educational extension of advanced language skills. Assessment may be helped by the fact that the child’s parent or near relative has often had similar problems in their learning.
Another question is whether or not it is always necessary or possible to discern the cognitive and emotional factors behind a learning problem. Difficulties in learning are often accompanied by several other simultaneous difficulties. For example, emotional problems may be either independent or consequences of the child’s learning disabilities. Additionally, emotional problems can sometimes produce problems in learning. It is not always possible to uncover the relationship between the difficulties, but even in such a case, it is important to plan sufficient support, which at its best provides diagnostic information, and to ensure follow-up.
References
Atkinson, J. W. & Raynor, J. O. (1974). Motivation and Achievement. Washington: John Wiley &
Sons.
Baker, C. (2003). Foundations of Bilingual Education and Bilingualism. 3rd Edition. Clevedon:
Multilingual Matters.
Christenson, S.L. & Ysseldyde, J.E. (1989). Assembling student performance: an important
change is needed. Journal of School Psychology, 27, 409-425.
Frith, U. (2001). What framework should we use for understanding developmental disorders?
Developmental Neuropsychology, 20, 555–563.
Gachathi, P. (1976). National Committee on Educational Objectives and Policies. Nairobi: Government printer.
Horowitz, F.D. (1992). The risk-environment interaction and developmental outcome: A theoretical perspective. In C.W. & J.G. Auerbach (Eds.), Longitudinal Studies of Children at Psychological Risk: Cross-nationalperspective. Norwood, NJ: Ablex Publishing Corporation.
Kuutondokwa, S. (2003). Reading Difficulties in Lower Primary Rural Areas Schools. Fieldwork
Report: University of Namibia, Windhoek.
Meltzer, L. (1996). Strategic learning in students with learning disabilities: The role of self-awareness and self-perception. Advances in Learning and Behavioral Development, 10B, 181–199.
Marope, M. T. (2005). Namibia Human Capital and knowledge Development for Economic Growth
with Equity. World Express, African Region.
Mbenzi, P. A. (1997). Analysis of reading Error patterns of Grade 5 learners at Namutoni Senior
Primary School and how to overcome them. Fieldwork Report: University of Namibia, Windhoek.
Ministry of Education. (2005). Lower Primary Phase Syllabus, English First Language.
Ministry of Education. (2009). Education and Training Sector Improvement Plan (ETSIP). [Online]. Available: http://www.mec.gov.na/ministryOf Education/etsip.htm [2009, June 27].
Nepando, J. T. (2003). Reading Problems Experienced by Selected Learners in Selected Schools in
Namibia. Fieldwork Report: University of Namibia, Windhoek.
Ondiek, P. E. (1986). Curriculum Development: Alternatives in Educational Theory and Practice.
Nairobi: Lake Publishers and Enterprices.
Republic of Namibia, (2003). 2001 Population and Housing Census National Report, Basic Analysis with Highlights. Windhoek, National Planning Commission.
Reynolds, D. (1997). School effectiveness retrospect and prospect. Scottish educational Review,
29, 87–113.
Rourke, P. & Del Dotto, J. (1994). Learning Disabilities. A Neuropsychological Perspective.
Thousand Oaks: Sage Publications.
SACMEQ. (2004). A study of the conditions of Schooling and the Quality of Primary Education in
Namibia. By D. K. Makuwa, National Research Coordinator.
Sinalumbu, F. S. (2002). Examining Reading Difficulties of Grade 7 learners within a School in
Oshakati. Fieldwork Report: University of Namibia, Windhoek.
Wang, M.C., Haertel, G. D. & Walgerg, H.J. (1994). What helps student learn? Educational
Leadership, January, 74–79.

Mika Paananen, Pamela February, Kalima Kalima,
Andrew Möwes and David Kariuki
2. Learning Disability Assessment
Learning disability assessment begins at school
In Finland, assessment of the causes of learning disabilities usually begins when the parents (or other guardians) or the teachers are worried about the child’s learning progress (see Figure 4). This is usually followed by the special education teacher’s assessment. In cooperation with the class teacher, the special education teacher evaluates, for example, whether the child has difficulties in reading, spelling, or mathematics. In Finland, the special education teacher can also quite precisely determine how extensive the difficulty is and what kind of support the child needs. When the teacher’s evaluation seems insufficient and additional help is desired in planning support, the child or adolescent can be referred to the school psychologist, family counselling centre, or health centre for further assessment. This further assessment is necessary when
• in spite of diligent work and special education services provided, the child does not learn according to expectations;
• the school’s own evaluations and assessments do not seem adequate (for example, there is reason to suspect an extensive problem that the special education teacher’s methods failed to assess);
• the school requests assistance in planning appropriate educational support;
• the school requests assistance for smoothing out disagreements between the school and the home;
• the family, teachers, or the child are worried about changes in the child’s learning;
• clear regression has occurred in the child’s skills;
• an appraisal is required of the need for support and intervention services from a party outside of the school.
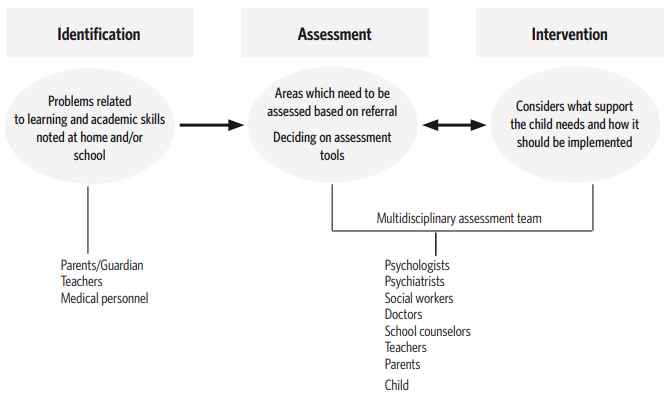
Figure 4. Multidisciplinary approach to assessment and intervention of learning disabilities
In Zambia, for example, the process of assessing learning disabilities, at its highest level uses a similar format to that in Finland. Most of the problems are initially spotted by parents when their child is not making adequate progress in school. In some instances, the teacher may notice that the child is not making adequate academic progress and subsequently asks the parents to consider taking the child for assessment. The teacher may also contact the assessment personnel directly and request for an assessment to be conducted, which would of course only take place with the consultation and permission of the child’s parents. Currently, Zambia’s Ministry of Education has a policy to ensure that children are assessed in order to determine their specific needs before they can be placed in a special school. The Ministry even makes some of the referrals to the assessment centre where a detailed assessment can be made. There are other instances when doctors at the paediatric and mental health hospitals send children to the assessment centre to determine the level of functioning of the children. At the paediatric clinic, the assessment often aims at establishing the learning needs of the child. The referrals to the mental health hospital are often children with special needs who may have been abused or defiled, in which case the courts require an assessment in order to establish the child’s functional level.
Needless to say, there is quite a large variation between the African countries with respect to the available resources and the way educational policies are applied in terms of identification, assessment and intervention, but what is common to all these countries is the need to do more for children who have a learning disability. In Zambia, most of the children with learning disabilities are “diagnosed” without necessarily undergoing a proper assessment. To improve this situation, assessments should be made mandatory by law for the benefit of all children before they are placed in special schools. However, in Zambia, the services of psychologists are not available for many people since, to a large extent, psychologists are found only in the capital city of Lusaka. It is therefore imperative to decentralise the services of psychologists in order to also make them available at provincial and district levels. Currently, the idea of having a multidisciplinary team including a psychologist, a school doctor and a trained special education teacher to deal with children’s early assessment is still a dream in many African countries. Furthermore, in African countries, most assessment instruments that are currently in use for the diagnosis of learning disabilities are standardised using Western norms. This raises ethical issues as a lack of sensitivity to cultural differences can result in misdiagnosis or mislabelling. More effort should be made to standardise assessment tools to include the local norms.
Assessments by classroom teachers and special education teachers
Early childhood has been recognised as a crucial stage in human development, not just in African countries, since it forms each individual’s foundation for subsequent development and learning, further underlining the need for more educational resources. Early identification of special needs in young children is a process or service that has gained popularity in recent years. This is because it is hoped that it will be easier to prevent serious problems and reduce the impact of a disability at an early stage of development. Identifying problems in young children is not always an easy task, but it is a worthwhile to undertake, especially for the purpose of preventing more serious difficulties from occurring later on.
The identification of learning related difficulties begins already when a teacher has a feeling or intuition that something may be wrong with a child, or that a child does not perform according to his/her best ability. It is then the teacher’s duty to investigate that notion in order to confirm or refute it. In such a case, initial identification of learning related difficulties is primarily based on the intuition of the teacher. Intuition, however, is always based on something – it is not simply a matter of coincidence, but arises from a knowledge and insight concerning the child’s educational situation. Factors heightening a teacher’s intuition include dedication and empathy, which motivate the teacher’s interest in each student within the class. Teachers should never regard any worrying behaviour or comments by students as coincidental, but should always try to relate them to possible problems that the child might be experiencing at school or at home, as these problems may affect the child’s development towards adulthood. However, teachers should take care not to misunderstand a student either, as this could cause them to label the child incorrectly as a person that he/she neither is nor wants to be. Teachers should therefore seek to find concrete evidence to support their intuition by systematically observing the child in different situations.
Sometimes parents are the ones who may suspect that their child has certain problems or special needs, leading them to mention these to the teacher for further investigation. Parents who are interested in their children are seldom wrong in their intuition about problems that their children might be experiencing. However, the combined intuition of both teacher and parents does not constitute sufficient grounds for a confirmation of the child’s special educational needs. There are three basic skills that teachers should master before they can successfully identify any problem a child has, namely observation, screening, listening, and questioning.
Observation: Observation can be explained as a “visual inquiry conducted through systematic observation.” Teachers should begin their observation without any preconceived ideas about the children in their class. By minutely observing children’s behaviour in the classroom, on the sports field and during other extramural activities, one can conclude whether a child manifests any unusual behaviour. In the classroom, the teacher should note whether a student’s current behaviour differs from his/her normal behaviour. This also applies to conversational situations and working sessions. The teacher may ask him/herself, “How does the child act towards other learners?” or, “Does the child behave differently in different situations?” A child’s nonverbal communication with the teacher and other students, as reflected in body posture, facial expressions and gestures, should also be carefully observed to determine the nature of the child’s emotions within the learning environment.
Additionally, teachers should be aware of serious or even mild ailments a child in the classroom may suffer, such as relating to asthma and migraine, impaired vision or hearing, epilepsy or motor coordination problems, as well as malnourishment or undernourishment. The sooner these conditions are identified and the affected children receive treatment, the less impact they will have on the child’s achievement in school.
Screening: Screening is a technique for acquiring information about a great number of people in as quick a time as possible. The results of tests and examination papers can be used as screening methods to identify those children whose results are poorer than they were expected to be. It may be that a child is diligent in class (e.g., first to answer questions) but does not perform well on examinations. Such a child may be singled out for further diagnosis.
The psychological assessment
The psychological assessment is more extensive than the teacher’s pedagogical assessment, and it seeks to understand the child’s learning difficulties in relation to the his/her entire cognitive performance profile and earlier development. This makes it possible to detect and exclude other factors that affect learning (e.g., more comprehensive developmental problems, environmental factors). Learning disability assessment may be an independent process or part of a broader analysis by the psychologist of the child’s life situation, including evaluating the development of the child’s emotional life and personality. Additionally, a well-trained special education teacher can also perform a comprehensive learning assessment. The extent of the assessment to be performed is determined by how problematic the child’s situation is felt to be, how multifaceted the problems seem, and by the results of earlier assessments, which usually help to direct and focus the current assessment questions.
In addition to the overall extent of the assessment required, its nature is determined by the child’s school history at the time in which the assessment is to take place. If the child is assessed when there is yet but a mere suspicion that he/she is not learning at the same pace as his/her peers, the results are likely to show that the difficulties have not necessarily affected the child’s life very broadly thus far. In such a case, the learning disability’s effect on the child’s self-esteem and school motivation may only be minor. But if the assessment is to take place when the child’s difficulties are already evident to such a degree that there is great concern over e.g., his/her progressing to the next grade, then the type of assessment needed will be of a different nature. In such a case, the parents may already know a lot about their child’s difficulties and many forms of support may have already been tried at home and at school to support the child. The child may also be quite aware of the nature of his/her own learning difficulties and these may have already had considerable ramifications in the child’s life. Whatever the starting situation may be, the psychologist must, naturally, use his/her own judgement to consider the direction and extent of the assessment.
The learning disability assessment conducted by a psychologist can be divided into four different procedures, each of which requires gathering information from several parties:
1) assessment of the phenotype,
2) developmental history,
3) assessment of cognitive functions, and
4) modifying or intervening factors.
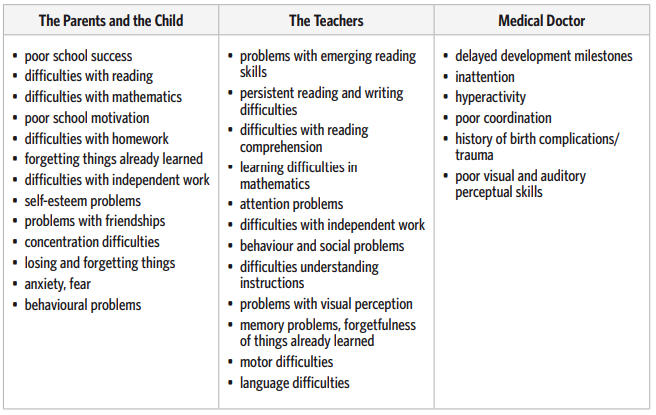
Phenotype: Learning disability assessment is usually begun with the procedure of examining the child’s functions and behaviour, or in other words, defining the phenotype problem (see Figure 5 and Table 2). A specific problem could be, for example, dyslexia, difficulties in reading comprehension, or attention problems. The description of the phenotype helps in choosing the right assessment method and facilitates time management. It is also important for choosing the most effective partnerships for cooperation, and it helps to target the assessment as well as the planning of the intervention.
Developmental history: The second standard assessment procedure is to examine the child’s development and its special characteristics and possible risk factors. Knowledge of the child’s developmental history offers more specific information about the history and possible causes of the difficulties or disability. Developmental history is often an important source of information, for example, in questions of differential diagnosis.
Cognitive functions: The third procedure is the assessment of cognitive functions and a more detailed evaluation of the problems detected in the phenotype. This offers detailed information on the nature and causes of the difficulties or disability. Cognitive functions and the assessment of academic skills are discussed in detail later in this book.
Modifying factors: In the fourth procedure, so-called modifying or intervening factors must be examined. These are the child’s environment and interaction with it, and the child’s own experiences. They modify how the problems manifest themselves in the child’s life, as well as determining the appropriate support. Assessing environmental and interactional factors reveals whether the support for the child’s skill level is sufficient or if more extensive support is necessary in the child’s life. The child’s own experiences ultimately determine how he/she reacts in different situations and how problems are interpreted depending on the child’s behaviour. Scientific research has revealed and classified different categories of learning disabilities and in most cases a child’s problem can be matched with some existing category or subcategory. However, the child’s temperament, personality and environment give the problems an individualised expression. Taking this into consideration whilst determining and making an assessment of the child is vital for understanding the whole problem as well as, in particular, for planning support.
Figure 5.The components of assessing learning difficulties (modified from Taylor, Fletcher & Satz, 1984)
Testing hypotheses in learning disability assessments
The goal of learning disability assessment is to provide information regarding the nature of the child’s learning difficulties, its causes, and above all, what kind of support the child needs. Following the model described above, assessment can be understood as a multilevel process. Each assessment procedure is conducted using different methods, providing different information. Together, the different sources of information create a general overview of the child’s difficulties. The assessment process has often been likened to scientific research, as justifiable hypotheses are made about the causes of the detected difficulty. These hypotheses are then tested with the information received on the different levels. The first hypotheses are made from the information in the referral and are expanded upon in the interview. The interview may already uncover new information that disproves one of the first hypotheses. Thus new hypotheses are formed, which are then tested in the assessment. Diagnostic assessment is a process in which reaching conclusions requires information from different sources. The nature and significance of each data collection phase is described in detail as follows.
Description of the phenotype problem. Familiarity with the phenotype of the child’s difficulties prior to commencing the assessment is important as it guides the assessment process. The phenotype description facilitates the choice of methods and time management. It also helps in choosing partnerships for cooperation and to add focus to the assessment and later support. Preliminary information about why the child has been sent for assessment and what problems have already been detected needs to be known before the psychological assessment can go ahead. At the onset of the assessment – preferably before the pedagogical or psychological assessment stages – it is good for those conducting the assessment to meet the parents and, if possible, the teachers as well. Parents can talk about how the problems are recognisable in daily life. It is essential to find out what kinds of conceptions and beliefs the parents have concerning the nature and causes of the observed problems and the child’s developmental history. Parents can also share information about the child’s hobbies, interests, and relationships with friends. At the same time, it is essential to find out the parents’ expectations in regard to their child’s learning, information about family interaction, and the amount of support the child is currently receiving (see Tables 2 and 3).
Table 2. Identification of learning disability phenotypes which cause parents, the child, teachers or the family doctor to be concerned
The school teacher’s as well as the special education teacher’s observations of the child are important for the psychologist to determine the phenotype. Teachers have seen the difficulties manifested in class and can share their expectations of the child’s learning potential. They also know about the child’s earlier learning experiences, strengths and weaknesses, working strategies and skill level. They are also aware of the forms of support having been provided. Mapping out child-teacher and parent-teacher interaction, the teacher’s attitude towards the child and the child’s difficulties, and the support available at the school all help in forming an understanding of the child’s classroom life and what type of support is necessary and possible. In Africa, the teacher’s role is mainly to provide instruction, then to evaluate the students in order to find out their level of achievement in relation to the curricular objectives. Evaluation is usually a combination of formative (continuous) and summative (end of term) processes. Feedback from these assessments is meant for use in making rational decisions when developing improvements. Many teachers are successfully able to modify the learning environment opportunities in order to assist the learners with difficulties. It is common for schools to reward students who do well in class, but there is a change, for example in Kenya, towards extrinsic motivators.
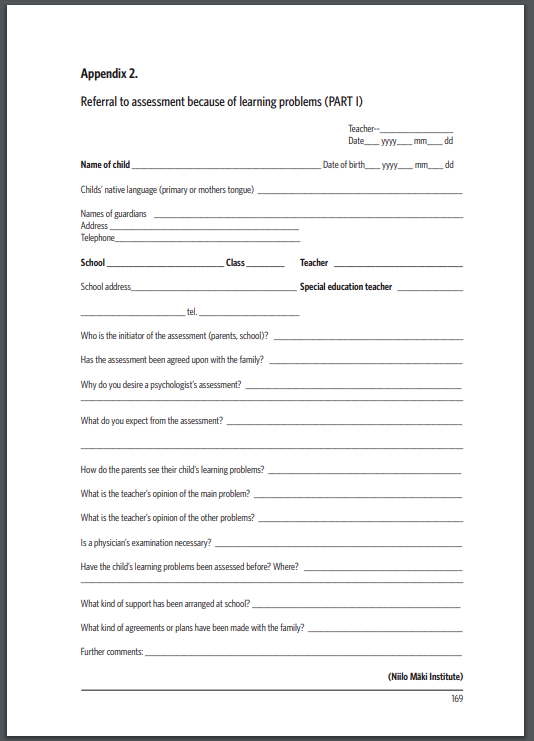
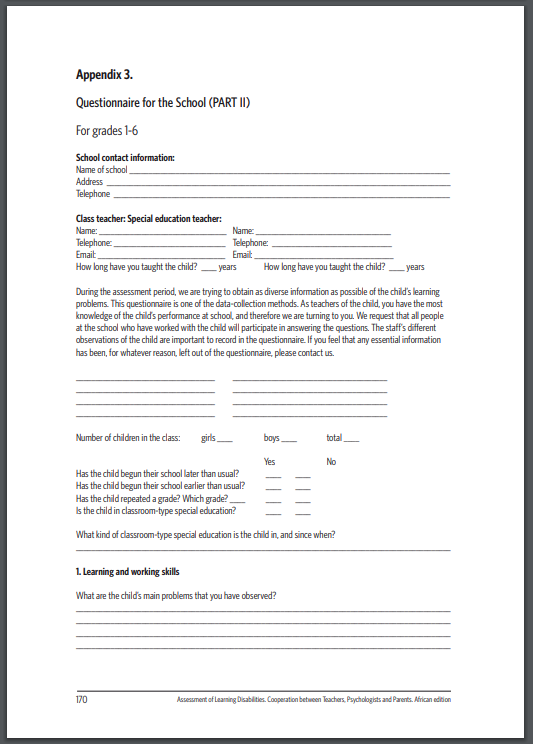
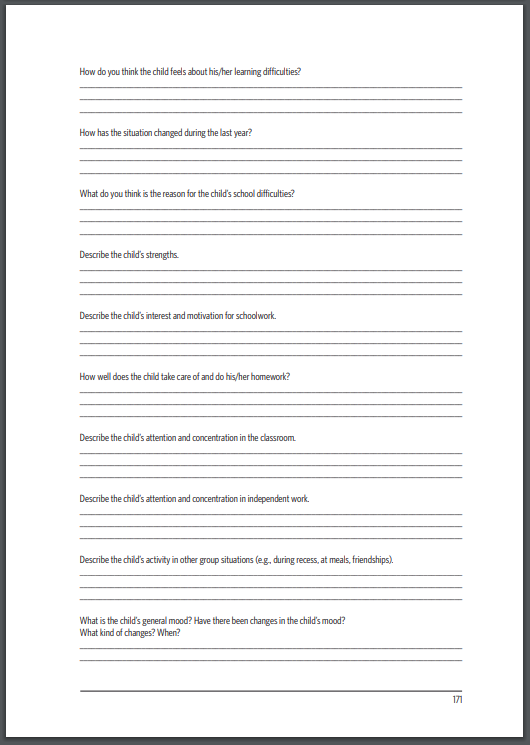
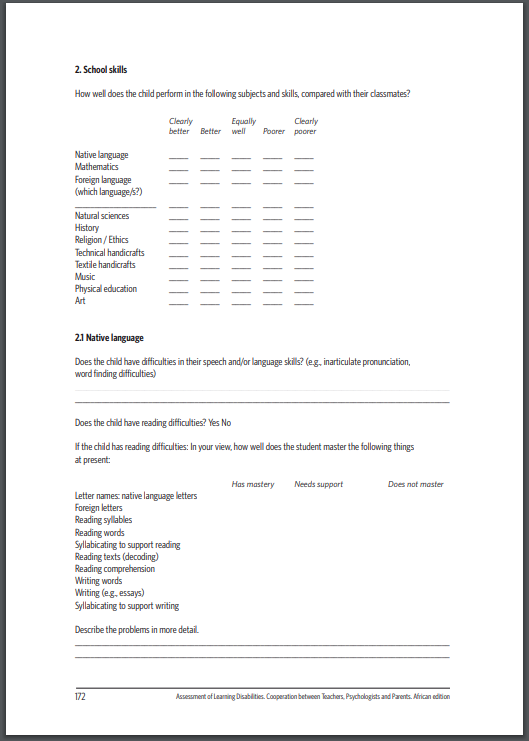
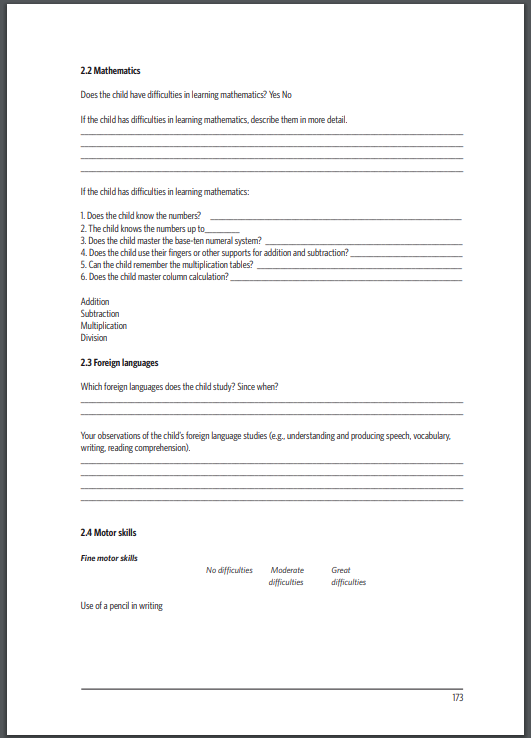
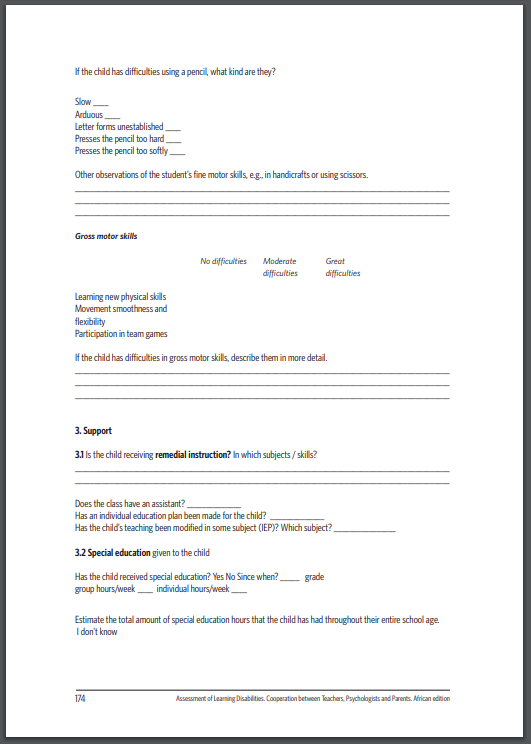
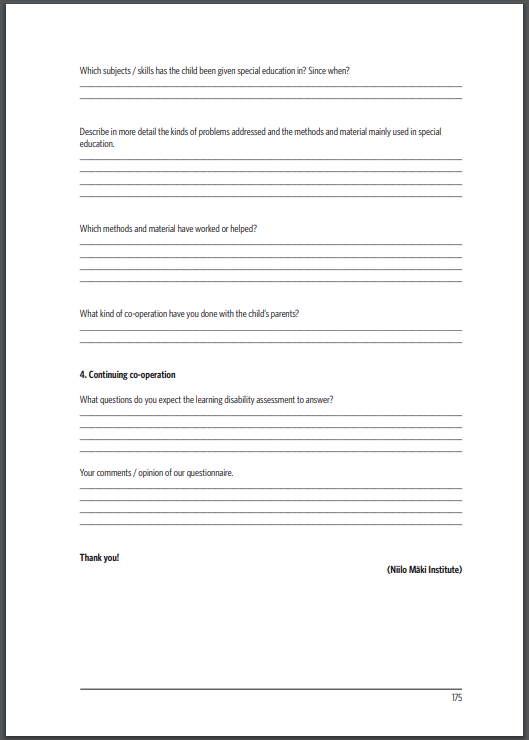
In Appendix 2. there is an example of a form that a school might use when sending a child to a psychologist for learning disability assessment (the form can also be found in the Appendix). In Appendix 3. there is an example of a form that can be sent to a school, from which the psychologist can then map out the child’s learning history, the child’s present situation, and the school’s expectations for the learning disability assessment.
Table 3. Examples of questions for describing the phenotype of the problem
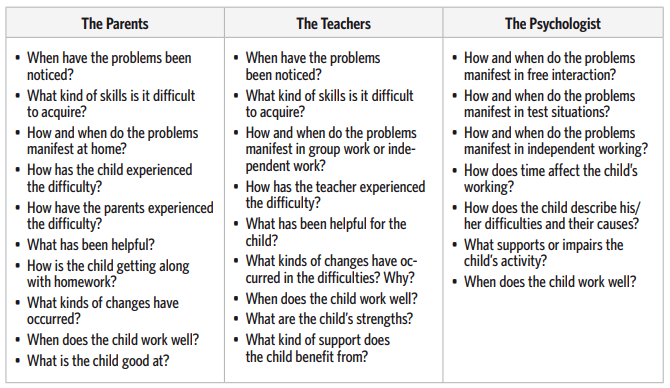
Gathering information concerning the child’s development. During assessment, a picture must be formed of the child’s skill development, the progress of his/her school learning, and earlier observed difficulties. Parents can often describe the child’s early development, and further information can be found in child health clinic records. Sometimes there are signs of comparatively slow skill development in the child’s developmental history. However, it is possible that the parents have not observed anything peculiar, or they do not recall any unusual characteristics in the child’s development. In such a case, it is the task of a professional to identify features in the parents’ descriptions that possibly point to atypical or slow skill development. Hence, the parents’ report of normal early development is not always a guarantee. The professional tries to identify the significant early characteristics of the child’s problems and to map out the development of the more slowly acquired skills (see Table 4).
Developmental steps, early signs of problems and risk factors are mapped out according to the child’s developmental history. Development data is information about, for example, the acquisition of motor, language and social skills, and about whether the child has developed according to expectations. Risk factors may be pre-, peri- or postnatal complications such as illnesses or accidents, which may have caused neurological problems or slowed down development. It is also useful to map out the child’s traumatic or stressful experiences (such as the death of a close relative or the parents’ divorce). These experiences can undermine the learning ability of some children, especially during the time of the highest stress. It is also necessary to ask for information regarding the parents’ and other close relatives’ learning history. Often the child’s father or mother has had similar learning problems and these characteristics have been passed down to the child. Information on how the earlier difficulties have been overcome or viewed in the family can help in understanding the significance of the child’s difficulties for the family, and to find means for the family to receive assistance and reinforcement.
Sometimes poor instruction can cause problems with learning and this should also be considered as we gather information about the child. Furthermore, it may also be necessary to gather information about the child’s academic history in terms of the frequency of changing schools. There are cases where the family is in denial about the child’s learning problems. They believe that the child’s poor performance is due to e.g., the failure of the school to teach properly. They move the child from one school to another hoping to find a school that will solve the problem that the child has.
Educational systems usually fail to meet the needs of the learner if the main goal of the educational planners is to simply classify learners into groups of good or poor performers. In Africa, some of the traditional problems with educational systems are
- placing too much emphasis on the subject matter without considering learners’ real needs, interests, problems and abilities;
- the subject matter takes too little account of the needs of the society, the learner, and the economic and personal challenges of the learners;
- the systems are very rigid and do not take the dynamic nature of the society and world into account;
- much educational practice is not in line with the needs revealed by research concerning child growth and development;
- the traditional curriculum is too academic, leaving little room for the consideration of learners’ individual differences.
In connection with these issues, many educational systems do not consider the developmental steps, early signs of problems, and risk factors in respect to the learners. If the child has been assessed before, then the current psychologist should obtain summary reports and copies of the previous psychologist’s test records. This eliminates unnecessary work as the reports reveal valuable information already gathered. They also show the plans made and implemented to improve the situation, as well as how these have affected the child’s development. When results obtained at earlier times are interpreted by the psychologist in the current examination, the significance of the repetition to the results must be carefully considered, especially if only one year or less has passed since the previous assessment. In the assessment of the actual change in skills, descriptions of the significance of situational factors and familiarity with the characteristics of the test are useful.
Most of the psychological or neuropsychological tests that are used in Africa are adapted from foreign versions in order to enhance their validity and reliability. There also exist locally devised assessment profiles, screening tools and checklists that meet international standards. It is hoped that with a growing appreciation of the benefits of sharing knowledge, more collaborative research and development of materials will take place in Africa.
Table 4. Examples of information concerning the child’s development
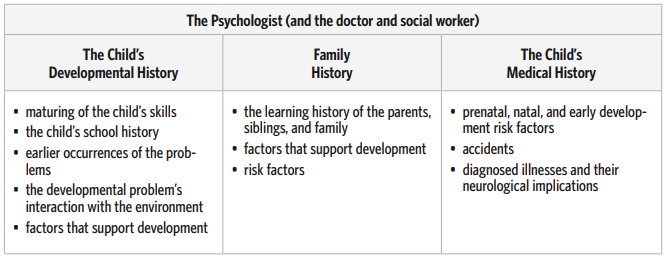
Assessment of cognitive functions and phenotype problems. A basic tenet in the assessment of cognitive functions is that the child’s overall activity consists of various subfunctions. Some of these may have developed below age expectations, which produces an observable problem phenotype. Some functions are clearly delimited and affect only certain operations (e.g., evaluating spatial orientation and directions, i.e., left-right, up-down). On the other hand, some functions are general and their deficiencies reverberate to many situations (e.g., maintaining attention). Assessing cognitive functions with tests provides information about the child’s weak and strong skills, upon which support and intervention can be planned for the child. It must be taken into account that any test’s capacity to tap into individual cognitive functions is limited. All test tasks demand more than one function simultaneously. To adequately determine the primary functional deficit, it is useful to do several elaborative tasks in the areas where weaknesses in learning or test tasks have been observed.
In addition to examining cognitive functions with different tests, it is necessary to consider the following points:
• Qualitative observations should be made of the child’s working rutines, attention, alertness, and following of instructions while working on tasks.
• The child’s emotions and self-efficacy beliefs, as well as his or her attitude towards the situation and the adult worker must be considered.
• The defence and coping mechanisms (e.g., avoidance behaviour) that the child uses provide information about the child’s means of coping with difficult situations.
• During assessment, the child should do schoolwork such as reading, writing and mathematical tasks as these can show the assessor how the child’s problems manifest themselves in practice (see Table 5).
Table 5. Assessing academic, problem-solving and cognitive abilities

Assessing modifying factors. The terminology “modifying/intervening factors” is used to describe how, in the end, such factors define and mould the way difficulties manifest themselves. These factors can pertain to the child’s environment, social relations, interaction and motivation. How the child experiences a situation and its difficulties is also such a factor.
The assessment situation is sensitive to the effects of the child’s emotions. The reactions manifested in test situations are often similar to the ones experienced by the child while doing tasks at school. Hastiness, depression, fatigue, fluctuating emotions, or the strong presence of defences affect the child’s task performance and this must be taken into account while interpreting the test performances. The child’s ability and means to cope with his/her problems are also affected by the child’s self-concept as a learner. This concept is formed and developed very early on in learning and teaching situations, as are the student’s subjective goals and interpretations of tasks. The child’s orientation in learning situations may also reflect his/her early childhood experiences of how the parents have instructed the child in various learning experiences and the emotions that were attached to these experiences.
In Finland, the researchers at the University of Turku have been interested in how a child’s task motivation can be deduced from their behaviour in task situations (Lepola, Salonen, Vauras, & Poskiparta, 2004). This approach guides parents and teachers to observe the child’s behaviour and to understand his/her attitude towards tasks, even when the children themselves cannot describe their feelings about themselves or their self-conceptions as learners. At least three types of orientation in children’s attitudes towards learning and instruction offered by adults can be distinguished, such as by focusing on the child’s behaviour, adaptive functions and feelings of self-efficacy.
A task-oriented attitude means that the child’s attention in a task and instructional situation is focused on the task itself and its challenges; the child approaches the task and, if necessary, the instructor as well, and the feelings he/she expresses towards the task and the instruction are positive. Successful experiences of instruction are believed to be behind such development, wherein the child has received appropriate amounts of instruction and support from an adult as well as opportunities to test his/her skills without too much fear of failure or excessive intervention by the adult, that is, the child has been given positive or neutral feedback concerning his/her performance. With the help of such experiences, children develop a strong sense of mastering tasks and trust more in their own task-solving skills. Working on and solving tasks should be rewarding for children.
A self- or ego-defensive orientation is seen as a negative attitude towards the task in the child’s verbal and non-verbal expressions (such as expressions of anticipating failure, tension and anxiety). The child may avoid tasks or instructional situations, or attempt to change the direction of events in order to avoid facing unpleasant or frightening situations. The child may also choose easy tasks, start fooling around or justify his/her failure (e.g., saying, “My hand was sore”). The reason for such action is that children, like anyone, do not experience a task and instruction merely from the viewpoint of the task, but they also perceive what the experience seems to say about themselves. Failure tells them not only that a task was difficult, but also that “I am not good enough.” The child tries to protect him/herself from such an experience (self-defensive attitude).
The child with a self- or ego-defensive orientation may have had experiences of insufficient and inconsistent instruction. Perhaps too much has been expected of the child concerning the given instruction and his/her skills, and they may have received, or felt to have received, negative feedback for their attempts. The child may feel that he/she has been left alone too often when facing overly challenging tasks, or that he/she has failed at attempts to solve difficult tasks. In task situations, this can lead to a child concentrating on him/herself or the instructor’s emotional reactions instead of on the task, and it can cause the distrust in oneself as a task-solver. In such a case, the child’s activity is superficial and unorganised.
A socially dependent orientation is seen in the child’s activity when he/she tries to follow the social clues of the environment and especially of the instructor, and relies on these in his/her decisions. In such a case, the child also actively gravitates towards instruction, for example, by acting more helpless than he/she actually is or by waiting for help or a hint from the adult. These children tend to be especially effective in getting help from others and they easily become overly assisted in proportion to their skills. Such children have an obvious need to be accepted and noticed. Instead of working on a given task, the child might approach the instructor for the sake of getting social attention even when he/she could complete the academic task without any assistance. The child has good social skills and evidently also knows it and enjoys receiving attention from the adult. However, often the child works superficially on tasks and learning may be based on imitation. The child may regard his/her own learning credulously, stressing social factors. Perhaps the child has previously received an overflow of instruction and support that has been overly directing and controlling. The child may not have had the opportunity to try out his/her skills sufficiently or to take responsibility for his/her decisions, and the attending adult has perhaps hurried to make the difficult decisions for the child. For this reason the child has not learned to take pleasure in solving intellectual challenges, but instead has learned to derive feelings of success purely from the apparent admiration and positive feedback he/she receives when gaining supportive attention from the adult.
The adult’s instructional practices affect how children’s conception of their own skills develops and what kind of problem-solver they see themselves as. At the same time, the child is an individual person and his/her temperament also affects the adult and the development of interaction already in early childhood. Certain children may have demanded much from themselves and their performance ever since they were little. Other children may have always been especially sensitive to feedback and have carefully observed their environment. Yet other children may have rejoiced in successes since they were a baby, regardless of the environment’s reaction. These characteristics affect the instructing adult and, together with the adult’s personality, the resulting interaction. One adult may be distressed in the company of a child who demands a lot of him- or herself and who closely observes the environment’s reactions. In such a case, the adult may minimise his/her own feedback, not wanting to reinforce the child’s tendency. Another adult with the same child might give him/her as much feedback as possible because the child seems to need it and seeks it. It is important for the instructing adult to understand the child’s way of looking at tasks and himor herself and the adult should also keep in mind that, through his/her own conduct, he/she can help the child to find an orientation that is productive for learning. However, this kind of instructional symbiosis often requires years of classroom interaction between teacher and child.
In learning disability assessments, it is important to gather information regarding the child’s social relations in addition to analysing their task orientation. Such information can be gained directly by observing the way the child interacts with his/her environment, and his/her inclination for making contact as well as activeness and flexibility. Acting in a social environment is affected by the child’s own natural tendencies, but also by the possible risks or supportive features of the stimulus environment and the family’s interactional practices. For example, in problems with verbal interaction, an explanation for the characteristic passiveness of children with learning disabilities has been sought in how different phenomena have been conceptualised and how the child’s inquisitiveness has been inspired in early childhood.
Social skills or ways of acting in social situations may be significant for diagnosing the child’s problems, such as in identifying Asperger syndrome. They also provide information about the protectiveness of each child’s social relations. This is especially significant for children with developmental and emotional difficulties. Because of the limited possibility to observe social skills in assessment situations, they are best evaluated indirectly, for example, by talking with the parents and teachers, observing the child at school, or by using a questionnaire (see Table 6).
Table 6. Social, Psychological and Educational factors affecting the child
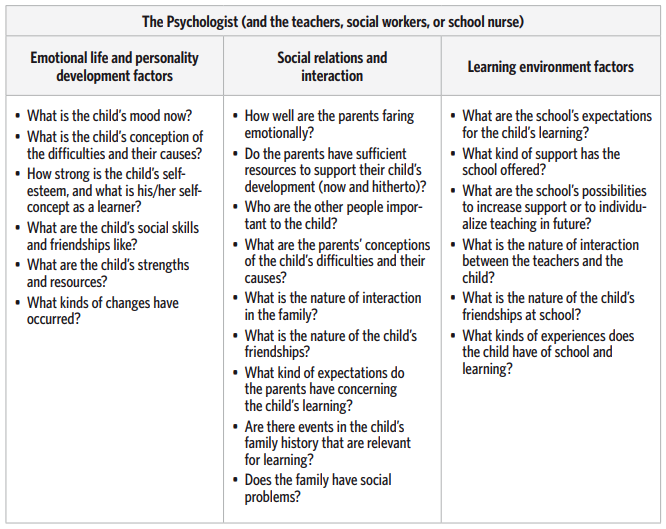
Examining circumstances that either support or impair learning is essential in assessing the learning environment. This leads us back to the observations presented at the beginning of the book, concerning the school community’s effect on the efficacy of the student’s learning. Assessment can focus on several levels: The school, the class, the teacher, and teacher-student interaction. Here it is possible to examine the amount, quality, and goals of the teaching and to evaluate how well it meets the child’s needs. Central issues in assessing the school are, for example, management and leadership (such as management vs. teaching personnel, control, and feedback practices), teaching arrangements, teaching groups and class size, the amount of teaching, the environment, and the atmosphere.
The teacher’s experiences, values, attitudes and expectations, particularly in respect to the student, affect how the teacher instructs the child and how their interaction develops. For the teacher as well, learning disabilities can often cause feelings of helplessness or even guilt. Teacher-child interaction may become negative, which causes discomfort for both of them and diminishes the possibilities for finding effective teaching and learning methods. It is thus important to examine teacher-student interaction in light of their mutual history and to consider how the positive aspects of their interaction could be supported. An essential part of planning support is to also consider the support that the teacher receives from the school.
References
Bessy, G. S. (1992). A Study of Curriculum Development in Kenya. Nairobi: Government printer.
Cameron R.J., Owen A.J., & Tee, G. (1986). Curriculum management (Part 3): Assessment and evaluation. Educational Psychology in Practice, 2, 3–9.
Kemp S. L., Kirk, U, & Korkman, M. (2001). Essentials of NEPSY Assessment. New York: John Wiley & Sons, Inc.
Lepola, J., Salonen, P., Vauras, M., & Poskiparta, E. (2004). Understanding the development of subnormal performance in children from a motivational-interactionalist perspective. International Review of Research in Mental Retardation, 28, 145–189.
Taylor, H.G., Fletcher, J.M., & Satz, P. (1984). Neuropsychological assessment of children. In G. Goldstein & M. Hersen (Eds.), Handbook of Psychological Assessment (pp. 211–234). New York: Wiley.

Nina Kultti-Lavikainen, Job Hengari, Beatrice Matafwali,
Sophie Kasonde-Ngandu, Grace Mulenga Kachenga and Mikko Aro
3. Reading and Spelling
How are reading and spelling disabilities manifested?
In Finland, the father of eight-year-old Sara contacted the school psychologist because the girl had met with difficulties in reading. In a consultation, the teachers told the psychologist that Sara was required to repeat the second grade. Yet, Sara’s schoolwork was going fine, that is, apart from her Finnish language skills. Her reading was slow and she made mistakes in spelling. Expressing herself was difficult for Sara. She raised her hand actively, but often when asked for an answer, she had forgotten what she meant to say. Sara understood what she read well. Her parents said that learning to write, and especially to read, had been troublesome for Sara. She had difficulties remembering letters. In the first grade, Sara learned to read short syllables, but even these took long for her to grasp. However, her father said he had marvelled at how well Sara could understand the text she read. But when Sara read out loud, listeners found it difficult to follow because her words broke at odd points and she might read the same word over and over again.
In Namibia, Peter, who was a six-year-old boy in a class of 32 children, lived with his father who adopted him from his mother after a medical officer informed him that the child was undernourished. His father completed grade 12 and had obtained a teaching diploma, in fact, he was employed as a teacher. At home there were no extra resources except the ones provided by the school. Peter had enough space at home, but learning facilities were not available. He also had enough food to eat at home. Peter spoke Otjiherero at home as his first language. The language of instruction at the school that Peter attended was English. He did not feel afraid and lonely at school, and even remarked, “I am a man”. He liked going to school, but didn’t want to show his school work to others. Peter said that he understood the language of instruction and favoured writing. He also liked reading, he said it was easy, and he understood and remembered what he read. He liked answering questions in class and participated in class decisions. He considered school tasks as easy and he did not have difficulties in remembering what was taught in school. He also liked to study when at home. The teacher rated Peter as weak in both oral English and in reading, and noted that he was far below the class average. The teacher considered him as not ready for school. Peter could not complete his school work without the teacher’s help. The teacher felt that Peter played too much in class and was not giving enough attention to his school work. According to the teacher, the school work was too much for Peter to cope with. Peter did not receive any special assistance from the teacher. The teacher talked to the father about the child’s learning problems, but the father was too busy and could not make time to help the child. The teacher considered the cooperation between the child’s parents and the school as nonexistent. The screening test for reading revealed that Peter had difficulty in learning how to read. His reading was characterised by refusals and showed that the child had limited “sight vocabulary”, as well as immature word attack skills.
In Zambia, Inonge was a seven-year-old girl who had just enrolled in grade 1. Her father worked as a messenger at a secondary school, six kilometres from home, while her mother was a housemaid in the neighbourhood. When her parents were away from home, Inonge remained with her grandmother. At home, Inonge had enough food and clothing but learning materials were nonexistent. Inonge’s mother had five miscarriages prior to Inonge’s birth, resulting in Inonge being the only child in the family. However, she was not lonely because she played with other children in the neighbourhood. After nine months in school, Inonge was still unable to read at a comfortable level. According to the teacher’s rating, Inonge was lagging behind the other children in class. She was unable to grasp the alphabetic principle and had substantial difficulties with letter-sound association as well as reading sight words. She was poor at taking notes, usually turned in incomplete classwork/homework, and performed poorly on tests. Given the high teacher-pupil ratio of the average class, one teacher per 55 students, it was practically impossible for the teacher to provide Inonge with special intervention. The teacher, however, summoned Inonge’s parents to the school to discuss the child’s situation. From the discussion, it was established that the parents were to provide additional support to Inonge.
In Kenya, John was eight years old while in the 3rd grade of a school on the outskirts of Nairobi. Instruction at his school was in English, although all students were expected to take one Kiswahili language course. He was the first born with two siblings aged six and four years. He was referred to the Kenyatta University Neuropsychological Centre by a teacher at his school. The referral comments were as follows: John was a very active child in and out of class. His playing interests were normal and typical for his age, and he preferred to play with same-gender children. He was very good at drawing. However, when it came to the time for reading exercises, other students mocked him for his slow performance. He made many mistakes in decoding words and was always at the bottom of the class at the end of term. Since the school did not have learning support programmes for slow learners, John’s father hired a private tutor. John only performed poorly in those subjects that require reading, including Kiswahili. A diagnostic assessment at the clinic, revealed that John had a specific reading disability without comorbidity.
These case studies point to the recognition that while reading as a skill is acquired in a relatively predictable way, a substantial number of children (like Sara, Peter, Inonge, and John) find learning to read a formidable challenge. There are a number of factors that may impede reading development in children, such as genetic and environmental aspects. Typically, a child with difficulties in learning to read may be slow to learn the names of letters; connecting phonemes to each other can be troublesome for the child. After learning basic decoding skills, their reading does not become fluent in pace compared to their classmates. Even after the child has strenuously studied, reading may be slow or flawed, or both.
The term dyslexia is often used to refer merely to a difficulty in reading, but sometimes spelling difficulties are included as well. Difficulties in reading and writing are often comorbid. However, they may also occur separately, in that the child may be proficient in one skill but clearly deficient in another. Reading difficulties appear in reading that is slow, flawed, or both. Spelling difficulties, for their part, appear as spelling that is incorrect, slow, or both (see Table 7). The issue of literacy development in the early years of schooling is a topic of inquiry that has received much attention in the recent past, also in many African countries. This is simply because recent studies have shown that a good number of, for example, Zambian children are reading below the expected grade level (Matafwali, 2005; Kalindi, 2006; Ojanen, 2007), and far too many are at potential risk of being conventionally classified as reading disabled (Matafwali, 2010). A study by Matafwali (2010) regrettably revealed that children hardly make progress in literacy development in the first two years of schooling. Similarly, results from a larger survey conducted by the Southern African Consortium for Monitoring Educational Quality (SACMEQ) on the conditions of schooling and the quality of primary education in Namibia has demonstrated that little success has been achieved in improving the quality of education, especially at the primary school level. It is against this background that disentangling myriad factors becomes imperative in order to explain the persistently low literacy levels of many African children and thereby increase the chances of early intervention for children at risk.
Table 7. The appearance of reading disabilities at home, at school, and in the psychologist’s
assessment

Development of reading and spelling skills
Children are often interested in written language already before receiving formal teaching in reading and writing skills. Learning word recognition and decoding skills progresses in stages. At first, children learn the respective names and phonemes of letter symbols. After that, they connect phonemes into syllables and syllables into words. Gradually, phoneme connection increases in speed and the child can fluently translate written language into phonetic form. Especially in languages with high letter-phoneme correspondence, the basis of fluent literacy is what is called “decoding”, or reading based on phonemic assembly. With decoding skills, the reader can combine phonemes into syllables and syllables into words, and can thus read words he or she has not learned before.
Spelling skills also progress in stages. Spelling is often assessed with dictation tasks. The child must first analyse the auditory perception and recognise the individual phonemes in the word. In the early stages of learning to spell, the child often repeats the word or an individual phoneme in the word to facilitate phoneme analysis. Once the child has recognised a phoneme, he or she can translate it into a respective letter symbol. For the child to translate the phonemes into letter symbols in the correct order, he or she must be able to process words serially. Finnish words are typically long and consist of several letters and syllables. In Finnish and other languages with regular phonemespelling correspondence, the abilities to syllabicate words according to the writing system, and to combine syllabication with written language, are important in both reading and writing.
Word recognition and decoding skills, as well as correct spelling skills, are tools of communication and learning. For the child to benefit from learning to read and write, he or she must understand what he/she has read, and he or she must be able to express his/her thoughts in such a written form that others can understand what he or she is trying to say. If the child has difficulties in reading comprehension or writing despite having mastered word recognition and decoding, the root cause may be, for example, problems in understanding the language or in directing and organising his or her own funsctions.
Box 2. Learning to read in different orthographies
In recent decades there has been an increased interest in comparing reading developments between different alphabetic orthographies. Research has tried to identify the effects that differences between alphabetic writing systems might have on the development of reading skills, or on problems in this development. Orthography (writing system) is a central concept when discussing cross-linguistic aspects of reading. The term refers to the set of symbols used to write a language and to the set of rules describing how these symbols are read or, respectively, spelled correctly.
Orthographies differ according to several aspects. Firstly, the phonetic components are represented with graphic or alphabetic symbols. Secondly, written symbols may represent syllables, consonant sounds, or all phonemes of the language. And thirdly, the orthographic code may also include nonphonetic clues such as morphological information. Most Western orthographies are based on alphabetic symbols that represent the phonemic level of the spoken language. Alphabetic orthographies with simple and straightforward correspondences between phonemes and graphemes are often referred to as “regular” (transparent, shallow) orthographies, whereas orthographies where the rules governing the mappings between letters and sounds are more complex are regarded as “irregular” (opaque, deep). Orthographic regularity is best defined as a continuum where English sits at the irregular end, and languages like Finnish, Italian and Spanish at the regular end. English has more than 40 phonemes and many more (often multi-letter) graphemes which may represent these spoken sounds in script. Finnish, a highly transparent orthography, consists of mainly single-letter graphemes consistently representing the 24 phonemes of the language.
There are over 73 local languages in Zambia, and seven of them (Nyanja, Bemba, Tonga, Lozi, Kaonde, Luvale and Lunda) have been officially designated as curriculum languages for the purpose of initial literacy instruction. In Namibia, 13 languages are used in instruction. There are over 11 indigenous languages in Namibia; including the Bantu languages such as Oshiwambo (spoken at home by 48.5 % of the native population), Rukavango (9.7 %), Otjiherero (7.9 %) and Silozi (5 %), and the Khoesaan languages including Khoekhoegowab (11.5 %) and Bushman (1.2 %). Some Bushman languages (e.g., Naro, !Xóö) are in danger of becoming extinct. In addition, some Indo-European languages are spoken in Namibia. Zambian languages, just like the Finnish language, are orthographically very transparent, which basically implies that they have consistent, regular and predictable correspondences between units of spoken and written language, on the level of single letters. Open syllables, like ‘ba’, ‘ta’, ‘ko’, ‘mi’ are very common in most words of the Zambian language, and clusters are rare. Of the indigenous languages used in Namibia, the ones of Bantu origin are mostly orthographically transparent. Similarly, Kenya has 46 tribes, each of which has its own language; it is noteworthy that the teaching is in English from the very beginning and that the majority of children are never exposed to reading material written in their mother tongue. About 90 % of the tribal languages in Kenya lack any printed materials, with the official languages being English and Kiswahili. Kiswahili is highly regular in comparison to English. These aspects all have implications for children learning to read.
The findings (e.g., Aro, 2004; Aro & Wimmer, 2003; Seymour, Aro, & Erskine, 2003) of crosslinguistic studies on learning to read consistently show that reading development is dependent on the language and orthography. The differences observed in the rate of reading development between children learning to read in different ortographies are best explained by differences in the regularity of the grapheme phoneme correspondence systems. Research suggests that there is a threshold on the regularity continuum that affects the processing requirements for initial reading. If the orthography satisfies relevant criteria for simplicity, early reading can be based solely on alphabetic processing – decoding is based on grapheme-phoneme correspondences and serial assembly. If the boundaries of simplicity are exceeded, the cognitive architecture of the reading process is different and a certain level of dual processing is required – decoding and whole-word based strategies. This would suggest that when learning to read, the regularity of grapheme-phoneme mapping has an effect on the difficulty of the task at hand. In regular orthographies, like in Finnish and many African languages, a child who has gained mastery of all letter sounds has the building blocks necessary for pronouncing practically any written word – in decoding, there is no need to pay attention to multi-letter units since graphemes consist of single letters and the correspondences are not dependent on the specific item or the orthographic context. Decoding can thus be taught and learned as a serial phonemic assembly of single letter sounds. In more irregular orthographies, as in English, a serial phonemic assembly at the level of single letters often proves unreliable as a tool for achieving correct pronunciation. Single letters correspond to a number of phonemes, graphemes often consist of multiple letters, and the reader has to pay attention to multi-letter segments while decoding.
Some findings also underline the possibility that the observed differences between orthographies reflect qualitative differences in the challenges facing the beginning reader in learning different orthographies. There might be some orthography-related variation in the salience of the different linguistic skills underlying reading development, consequently resulting in reading problems, although the neurobiological background of reading problems (dyslexia) seems to be shared. It seems that the development of phonemic awareness is supported by regular writing systems, where the phonological structure is explicated and transparent in script (Mann & Wimmer, 2002). Given the low literacy levels in many African languages despite relatively transparent orthographies, we are inclined to think that there are other serious challenges related to multilingualism, the quality of teacher education or instructional methods and materials, and possible confusion created by the multiplicity of several languages and orthographies one is required to master at school.
Cognitive skills related to difficulties in reading and spelling
The underlying causes for difficulties in reading and spelling are still partly unclear, but the modern understanding is that hereditary factors have a major role. More than half of the reading skill level variations are presumably due to heredity. However, heredity alone cannot explain reading and writing difficulties and their degree of difficulty.
In assessing the cognitive factors behind reading and spelling difficulties, it must be verified if the difficulty is connected with extensive language difficulties. If such broad language difficulties are discovered in a reading difficulty assessment, then the possibility of a specific language impairment (SLI) diagnosis and a referral to a child neurologist, phonetician or paediatrician should be considered whenever possible. Often, the cognitive difficulties observed in the assessment of reading disability turn out to be narrow in scope. At the core of literacy acquisition, there are a number of factors that seem to hinder the development of these important skills, among the most essential ones being phonological processing skills, verbal working memory, rapid naming as well as lack of proficiency in the language of instruction, as discussed in more detail as follows.
Especially in the findings of studies performed with English-speaking children, the difficulty of phonological processing (or phonemic awareness) has become a major factor. Children with reading and spelling difficulties often find it harder than their peers, for example, to perceive, remove or exchange the phonemes of words, or to repeat non-words. By definition, phonemic awareness refers to the child’s sensitivity to discern and ability to manipulate the sound structures of oral language. In respect to skill level, phonemic awareness involves the understanding that a singlesyllable word such as ‘cat’, which is experienced by the listener as a single beat of sound, actually can be subdivided into beginning, middle and ending sounds. It also involves the understanding that individual segments of sound at the phoneme level can be combined together to form words. There is sufficient evidence suggesting that phonemic awareness is critical for the development of proficiency in reading skills, principally because alphabetic orthographies encode lexical entries more or less at the level of phonemes (Bus, Ijzendoorn & Marinus, 1999). Generally, an awareness of phonemes is necessary in order to grasp the alphabetic principle that underlies our system of written language or orthography. Phonemic awareness skills also help children to learn to use letter-sound knowledge in order to read and build words. Conversely, children who have poor phonemic awareness skills in the early stages of literacy development are likely to experience substantial difficulties in reading at later stages in primary school and beyond.
It should be noted, however, that phonological skills and literacy have a reciprocal relationship. Phonological skills forecast the development of literacy, and literacy contributes to the development of phonological skills. Phonological skills alone cannot explain why learning to read is slow for some children. Deficits in processes of working memory have also been considered in connection with phonological difficulties. Especially the so-called immediate retrieval of language content is often harder for children with difficulties in learning to read.
Another skill central to literacy seems to be the ability to retrieve familiar words quickly from long-term memory (i.e., rapid naming ability). Difficulties in this area appear in assessment situations when the child struggles to name familiar symbols, such as colours or letters, quickly in succession. Children at risk for reading disabilities have previously been noted to have such trouble with rapid serial naming already around four years of age (Puolakanaho, Ahonen, Eklund, Leppänen, Poikkeus, Tolvanen, Torppa, & Lyytinen, 2007). The connection between rapid serial naming problems and reading/spelling difficulties is especially evident in the transparent languages. This relationship has also been established in Zambian languages, in regard to which Matafwali (2010) found that the rapid naming was a strong predictor of literacy outcome in children learning in Zambian languages in the first grade of school – even when the effects of oral language were taken into account.
Assessment of reading and spelling skills
It is important to assess the child’s literacy by listening to him or her read and by making observations as he/she writes. In reading assessments, both word lists and text should be read. Attention must be paid to reading fluency and mistakes made. Also to be assessed is the child’s ability to recognise letters and to connect these into syllables which are then to be connected into words.
Spelling should be assessed with both dictation and story writing. The teacher or psychologist should also uncover whether the child knows the corresponding letters of sounds, can discern the phonemic structure of the language, and is able to identify individual phonemes from words. In both reading and spelling assessments, it is good to observe the child’s ability to syllabicate both spoken and written words. It is important to ascertain whether or not the child can find the syllabic rhythm of words, and whether he or she has learned to syllabicate words according to the writing system as well. In addition to language skills, the child’s fine motor skills should be considered in making an assessment.
Special education teachers have assessment methods at their disposal with which they can compare the child’s literacy with the class level. Usually, mere observations of the child’s literacy are enough to reveal whether or not there are deficiencies in his or her skills. A closer examination, however, reveals the specific stage at which the child is in his or her development, the type of strategies being used and what kind of support is needed.
Learning reading and spelling skills requires the mastery of several cognitive functions, and if necessary, the psychologist can define the child’s cognitive skills more extensively whilst assessing the child’s literacy. Skill assessment is necessary to understand the difficulties behind a child’s dyslexia. This helps to understand the causes of dyslexia and its connection with the child’s other possible difficulties and strengths, and it also helps in planning teaching and remediation.
To find out if the child has dyslexia (a rather limited diagnosis) or more extensive difficulties, the child’s general cognitive functions must be examined. If the child has several cognitive difficulties, this probably also implies weaknesses in many important skills vital for learning to read and write. In such a case, it is important to concentrate extensively on planning teaching and remediation, not merely on strengthening reading and spelling skills. Discoveries based on clinical data reveal that there is no typical cognitive performance profile connected with dyslexia. Instead, we know well that at least minor language difficulties are often behind dyslexia. Hence, special attention should be paid to the child’s language development and language functions. When assessors examine language functions more closely, they try to discover whether the child has, for example, difficulties with naming, phonological processing or producing phonemes, deficits in working memory affecting language, or broader problems understanding words or phrases. Especially with older children, attention must be paid to skills in foreign languages and reading comprehension. These should be taken into account when planning support.
The following tables describe the stages of literacy and the difficulties typical at each stage. In the assessment column, we have described how each skill could appear in different tasks and in certain tests. References relating to tests can be found at the end of the chapter.
Table 8. Assessment of reading skills

Table 9. Assessment of spelling and writing skills
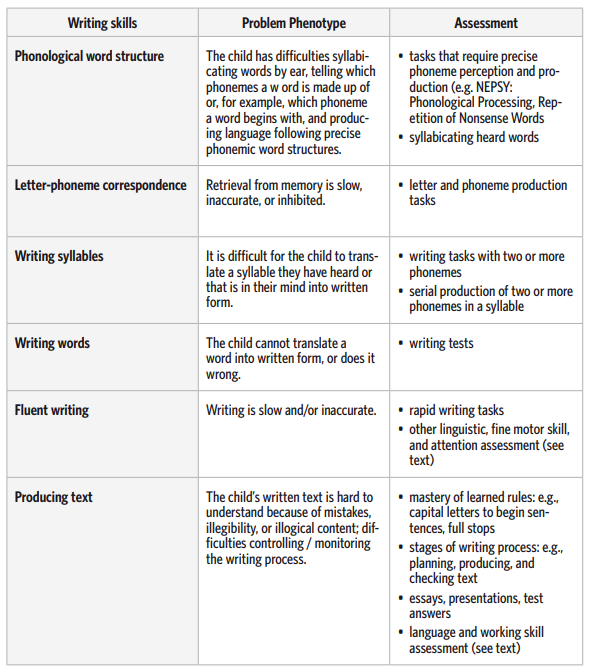
Table 10. ICD
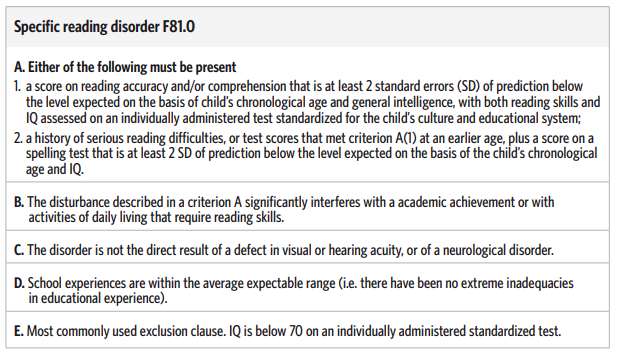
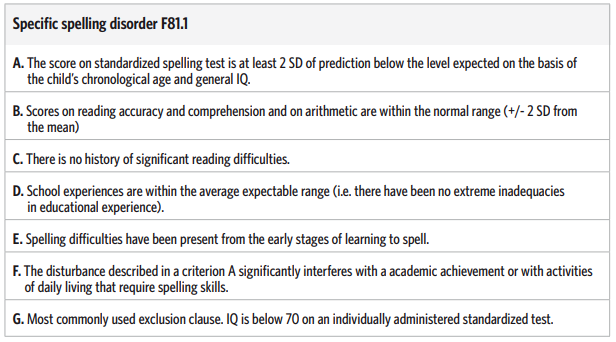
Language of initial literacy
Related to phonemic awareness, interest in the ways in which oral language facilitates initial literacy development in children has been growing in Africa during recent years. In Zambia, like in many other postcolonial African countries, English was chosen as the official language from 1965 to 1996. It was also used as the medium of instruction for all subjects from the very first day a child entered grade 1, despite the fact that it was not the mother tongue of the majority of the children (Kelly, 2000). Also in Namibia, as can be seen from the example of Peter in the introduction of this chapter, the official language (English) was opted as the medium of instruction in order to accommodate all learners with different home languages in the towns and cities. Moreover, there seems to be a great preference for English above the mother tongue as parents tend to send their children to English-speaking schools or even choose English as the instructional medium in schools that offer the option of teaching using the mother tongue. As a result, learners with primary language (mother tongue) skills struggle with the acquisition of basic English language skills, namely listening, speaking, reading, writing and spelling, having had only limited or, in some cases, no exposure to English (Mbenzi, 1997). Children arrive at school with varying levels of readiness for literacy learning, as in the case of Peter whose difficulties were indicated by his teacher. Peter seems to have picked up the wrong idea about what reading is, noted in his initial encounter with reading. There was a mismatch between Peter’s understanding of what a normative level of reading is and what the school expects of a good reader. It is important that teachers and learners alike understand the process involved in learning to read if we are to understand why some learners may sometimes fail to learn to read, and especially to find out how to better support children who fail to learn how to read.
Education in an unfamiliar language is assumed to be an enormous challenge for young children because they have to learn two complex skills simultaneously (Matafwali, 2010). Studies in literate societies have made plausible discoveries that a rather high level of proficiency in the language of instruction is required for children to benefit from reading instruction in school (Dickinson et al., 2003). Children in such a situation need to understand age-appropriate written texts that include more complex language requirements than is typical for daily communication in their mother tongue (Bus, van IJzendoorn, & Pellegrini, 1995). In light of this, the Zambian language policy meant that most of the children living there have been taught in a language with which they were relatively unfamiliar (Kelly, 2000). It is now argued that this approach compromised the quality of education being offered not only at the primary school level, but also at the higher levels. Drawing up the balance after thirty years’ application of this Zambian language policy, the results are negative: The policy did not succeed in developing adequate reading skills in children (Kelly, 2000). This is evidenced from the low reading levels among Zambian school children that have been documented in numerous studies (see e.g., Williams, 2004; SAQMEC, 2004; Kotze, Higgins, & Tambulukani, 1999; Kelly, 2000)
Research has clearly shown that the first thirty years of English as a medium of instruction had been less than satisfactory in promoting literacy development in Zambian children. A vast majority of Zambian children were struggling with learning to read and write. These unfavourable literacy levels in comparison with other countries in the sub-Saharan region prompted the Zambian government to usher in the Primary Reading Programme (PRP), with the New Breakthrough to Literacy (NBTL) as one of its major components. The NBTL is an adaptation of the Molteno project in South Africa, which was originally developed to teach functional skills to learners in their first language. It is an approach that brings the language that children are already experiencing in the home into the classroom, and the scheme works with children in helping them to recognise familiar spoken words when translated into a written code and to generate written language. The NBTL has recognised the important role of the mother tongue in the development of reading and writing skills.
Given the low literacy levels, we are inclined to think that although many African languages are relatively transparent in orthography, much like the Finnish language, the challenge still remains in a diversity of languages within a single country. For example, the aforementioned Primary Reading programme requires that children in grade 1 are taught to read in a familiar language, preferably the mother tongue. While this approach may appear straightforward in monolingual societies, implementing such a programme in a multilingual society like that in Zambia or Namibia is a formidable challenge, if not ambitious, considering their diversity of languages. It should be remembered, however, that there is evidence showing a nexus between oral language and phonemic awareness. Dickinson and colleagues (2003) have clearly shown that oral language is not only important for the acquisition of phonemic skills in grade 1, but that it is even more critical in respect to reading words. Based on this line of thought, children who lack proficiency in oral language skills are likely to have deficits in phonemic awareness, and it is these children who are at substantial risk of reading failure.
It is estimated that Zambia has more than 73 local languages, which makes choosing the local languages that should take precedence in education a mammoth task for curriculum planners. It is therefore not surprising that currently only seven local languages (Nyanja, Bemba, Tonga, Lozi, Kaonde, Luvale, and Lunda) have been officially designated as curriculum languages for the purpose of initial literacy instruction. This still yields the result that the majority of the Zambian children are learning to read and write in a language which is essentially not their mother tongue, though a greater number are now learning in their first language than was the case before the new programme. Studies in literate societies have shown that learning to read in an unfamiliar language is a recipe for reading failure (Snow, Burns & Griffin, 1998), especially for children who have not yet gained proficiency in the language of instruction, as may be the case for the majority of Zambian children.
Similarly to Zambia, Namibia’s native people also speak a variety of languages, in fact, over 11 languages are indigenous to Namibia. In public life, most Namibians are multilingual. Some children are exposed regularly to two (or more) languages from early childhood and thus – being truly bilingual – can be said to have two languages as a first language. Williams (2004) noted that it is commonplace in sociolinguistics that a language label such as ‘Oshiwambo’ or ‘Khoekhoegowab’ may actually encompass a variety of significantly different dialects or/and even consist of completely different languages, and that ”mother tongue” education is therefore not assured simply because the same label is attached to the language of instruction and the language of the learners. Obviously, the learners who lack adequate competence in the variety of languages used in education are at a disadvantage, particularly as concerns literacy skills. The languages spoken in Namibia are manifold, while in terms of linguistic relatedness or mutual comprehensibility, there are fewer. The Ministry of Education and Culture of Namibia carefully considered the views of diverse groups in formulating its language policy. The Ministry also made the following fundamental assertations (MEC, 1993):
• All national languages are equal regardless of the number of speakers or the level of development of a particular language.
• All language policies must consider the cost of implementation.
• All language policies must regard language as a medium of cultural transmission.
• For pedagogical reasons, it is ideal for children to study in their own language during the early years of schooling when basic skills of reading, spelling, and concept formation are developed.
• Proficiency in the official language at the end of the 7-year primary cycle should be sufficient to enable all children to be effective participants in society or to continue their education.
• Language policy should promote national unity
Like in many African countries, English is also the official language in Namibia. Until 1990, German and Afrikaans were official languages as well. At the time of gaining independence, English enjoyed government recognition and became the sole official language of Namibia to be used for all official purposes of the state, with the rest of the spoken languages recognised as national or local languages. Strange as it may seem, it is for a good reason that English is the only official language though it is the native language of less than 2 percent of the population. That is to say, during the era of Apartheid, the choice of a language was a “cultural right”, and this stance was used to legitimise divisions in the Namibian society, as well as the inequalities of power and privilege. Consequently, much of the public would have perceived the demand by any given group in the society for special consideration of their particular language to be an attempt to perpetuate the power and the privilege of that group, as privilege of the few was the practice before independence. Many local languages that are spoken by a significant number of people also fell short in printed materials for both instructional and leisure purposes, in some cases because these lacked a standardised orthography for use in schools or had limited terminology for some subject areas. In light of this, when crafting the language policy, there needed to be a fair balance between the abilities of individuals to choose their language of communication and the public interest in a common language to facilitate citizens’ participation and decision-making in a democratic society. Due to these considerations, the language policy in education came about as a compromise. English was considered as unifying the people and therefore took on a special place and function in education in Namibia. English came to be considered as a language of international connections and not foreign cultural domination. It is important to note that English, as in use in Namibia, is considered as “evolving”. Like all active languages, it changes as people use it. Beyond that, regionally specific variants of English have emerged. People in Australia, Canada and the United States of America are all proud of their national language, which they continue to call English even though it has diverged in important ways from what is heard in England (MEC, 1993).
In Namibia, English as a Second Language (ESL) is a subject for all learners from grade 1 through to grade 12 who do not have English as their home language. In general, English is the medium of instruction from grade 4 onwards. The purpose of English as a Second Language in grades 1-3 is to prepare the children for the transition to English as the medium of instruction in grade 4. The fourth grade is a transitional year in which the mother tongue plays a supportive role in teaching and learning. The purpose of English as a Second Language in grade 4 is to provide a careful transition from learning in the home language to learning through the medium of English (Ministry of Education, Lower Primary Phase Syllabus, Second Language, 2005). Thereby, Namibia has a bilingual policy model that is dominant in its primary schools. In some instances subtractive bilingualism (really meaning, English only) is practiced, while in other cases transitional bilingualism (early exit from use of mother tongue, see Chapter 1) is applied. Subtractive bilingualism is where the learning of a second language (in this case English) may undermine the person’s first language and culture (in this case the mother tongue), thus creating a subtractive situation. In a subtractive environment, the transfer of literacy skills between the two languages may be impeded. When literacy is attempted through the second language, the child’s oral skills in English may be insufficiently developed for such literacy acquisition to occur (Baker, 2003; Fleisch, 2008).
Reading and spelling disabilities, the environment, and interaction
Matafwali (2010) observed that children who experience substantial difficulties in learning to read and spell may constitute a special group within the education system that may, unfortunately, go unnoticed within the current educational provision in Zambia. She further argues that in spite of the Zambian government putting emphasis on the equity of access to education for children with special educational needs (Ministry of Education, 1996), there are currently no systematic procedures that have been put in place to ensure early identification and assessment of children who may be at substantial risk of developing reading and spelling difficulties. In this respect, it is important to recognise that although most children may respond to teacher-directed instruction in the normal classroom setting, a percentage of them will fail to advance with normal instructions and it is this population of children at risk that our educational system should be concerned about. Reading difficulties do not disappear overnight; thus, in the absence of intensive intervention, the gap between good and poor readers is likely to widen as children move up the educational ladder. In an effort to improve literacy levels, therefore, identification and assessment of children at risk should be strengthened both at school entry and at the classroom level. Matafwali (2010) observes that assessment of reading and spelling difficulties is “currently” not typically part of the Teacher Education training programmes in colleges in Zambia. Thus, professional development in this important area is vital so that teachers can be equipped with knowledge and skills regarding assessment of reading difficulties in order to be able to translate the results into more effective classroom instruction and intervention. It is strongly recommended that the assessment of children at risk of developing reading and writing difficulties should remain in the control of classroom teachers.
Reading and writing are basic skills that a child should master during his or her first few years at school, in order to be able to assimilate new knowledge and skills in the future. In Western societies, literacy is held in especially high esteem. At the onset of the first grade, well-meaning relatives and friends often ask the child, “Have you learned to read yet?” In the classroom, literacy is a concrete, observable skill that children themselves also compare among their peer group. Such well-meaning questions and comparisons with classmates tell the child clearly whether he or she can read or not. In the child’s mind, this often translates into a more extensive question: “Am I a good or a bad student?” or “Am I smart or stupid?” In this way, reading and writing skills, or literacy, play a vital role as the child forms his or her self-conception as a learner. Among the African indigenous people in Namibia, children are sometimes asked, “Have you started school?” and, “In what grade are you?” However, in many traditional societies in Namibia, literacy is not a practice and the natives do not often refer or make reference to reading and writing. Many natives practice oral culture, meaning they transfer their values, norms and culture orally from one generation to the next. Learning how to read and write is considered to be the responsibility of the school and the teachers. Whether you are going to be considered as smart and capable or a failure and incapable at school will be determined by the level of mastery attained by an individual learner in the basic skills of reading, writing and arithmetic.
Literacy is very important in both schoolwork and homework. As school years go by, the amount of texts to read and write increases. For a child with reading and writing difficulties, tasks take more time than for their peers. Sometimes this undermines the child’s belief in his or her skills and subsequently work motivation may be hard to find. Even though such a child may understand the given task instructions, often he or she needs an adult to help with reading. Upon being diagnosed with a reading or writing difficulty, to facilitate their learning, the child should be given special education, intervention, and special arrangements as soon as possible – and these should be continued as long as the student needs them, possibly throughout his or her education.
Therefore, to help students who are struggling with reading and writing, we must understand just exactly why these children are failing to read and write. We argue in this chapter that a substantial gap in language and phonemic awareness exists between poor and good readers. Accordingly, while reading and writing difficulties are developmental in nature, in the African context, it would be a mistake to assume that problems in reading and writing are limited to biological factors. In this section, we have demonstrated that myriad factors are responsible for low reading levels in the African countries. This brings us to the question of what instructional measures must be put in place within the classroom in order to help children at risk of reading failure. Are these children visible in the current educational practice? Are teachers adequately equipped with skills to meet the needs of children struggling with reading and writing in a diverse classroom environment?

Box 3. Graphogame and GraphoLearning Initiative
Heikki Lyytinen & Emma Ojanen
The University of Jyväskylä and Niilo Mäki Foundation have opened an initiative to collect efforts for support of reading acquisition among African children. Such support is necessary within the multilingual contexts that are affected by many factors which compromise the optimal opportunity to learn to read.
There are plenty of educational computer games available and more are developed for the expanding market. Graphogame is different for various reasons. First of all, it was scientifically developed for children who need extra help in learning to read, and it is not a commercial product (see the references). The most important part of the game is teaching letter-sound correspondences which are the basis for reading skill. The game itself has a very simple idea: a player hears speech sounds through good-quality headphones and sees a selection of written symbols moving across the screen. The player tries to catch a corresponding symbol with a mouse. If it was the correct one (“target”), player gets a score. If it was an incorrect selection (“distracter”), the same target item is repeated and provides the player a new opportunity to learn to connect the particular sound to its corresponding letter. Items are repeated in a different order and with different distracter options until the player is able to choose the correct symbols without errors.
This sounds simple, but instead of just providing learning material in electronic format, the game is programmed to provide specific contents for each individual player. The game is adaptable, which means that the game modifies the contents and speed according to the players’ performance level. When the player improves, the game items will appear on the screen faster and with more distracters. A less skilled one will have a slower game with fewer options on the screen. Each game level introduces new items which get gradually more difficult until the player is able to play with real words.
There is another feature that makes the Graphogame unique as an educational game. The Graphogame records the choices in each trial between the alternative written items after hearing the spoken item in each trial. These records can be examined at the Graphogame internet portal where researchers can access the information in a password secured website. These records (“gamelogs”) can be visualized as graphs by various in-built programs or the data can be transferred to statistical analysis on researchers’ computer. If children play with a computer that has an internet connection on, the data is updated at the server within mere 10 minutes after the child has played. Since researchers can access the data from the other side of the planet, the Graphogame provides an opportunity to collect data over long distances in a very short time. The data from gamelogs are used in reading research and development of better teaching methods and remedial programs for children with special needs.
The Graphogame can be adapted to different languages. The contents of the game are designed according to each language’s writing system and orthography. The game sounds need to be recorded with very good quality and they need to be phonetically correct for the language. Developing Graphogame adaptations to new languages provides interesting opportunities for language researchers, especially if the language is question is not widely known. Collecting data over internet also makes it possible to do cross-language studies and comparisons between children from different countries. All this is much needed in Africa.
The support that we are organizing in the Grapholearning initiative to African children attempts to reduce the detrimental effects of both of the above-mentioned bottlenecks. We will make available to the African countries a training game that operates within inexpensive phones as soon as its efficiency of instructing basic reading has been empirically demonstrated in each of the different orthographic environments. Furthermore, we aim to make exciting reading material available via phones to 7–10 year olds (see Grapholearning.info) to provide them with a basis for training functional reading skill.
References
Aro, M. (2004). Learning to Read. The Effective of Orthography. Jyväskylä Studies in Education, Psychology and Social Research 237
Aro, M. (2009). Effect of Orthography on Reading Acquisition – Theoretical and practical implications. DIEDUT,1, 9–21.
Aro, M. & Wimmer, H. (2003). Learning to read: English in comparison to six more regular orthographies. Applied Psycholinguistics, 24, 621–635.
Baker, C. (2003). Foundations of Bilingual Education and Bilingualism. 3rd Edition. Clevedon: Multilingual Matters
Bus, A.G., Ijzendoorn, M.H., & Pellegrini, A.D. (1995). Joint book reading makes for success in learning to read: a meta-analysis on intergenerational transmission of literacy. Review of Educational Research, 65, 1, 1–21.
Bus, A.G., van IJzendoorn, M.H.,& Marinus, H. (1999). Phonological awareness and early reading: A meta analysis of experimental training studies. Journal of Educational Psychology, Vol 91(3), Sep 1999, 403–414
Dickinson, D. K., McCabe, A., Anastasopoulos, L., Peisner-Feinberg, E. S. & Poe, M. D. (2003). The comprehensive language approach to early literacy: The interrelationships among vocabulary, phonological sensitivity, and print knowledge among preschool-aged children. Journal of Educational Psychology, 95, 465–481.
Fleisch, B. (2008). Primary Education in Crisis. Why South African schoolchildren underachieve in reading and mathematics. Cape Town: Juta.
Holopainen, L. (2003). Development in Reading and Reading Related Skills: A Follow-up Study from Pre-school to the fourth Grade. Jyväskylä Studies in Education, Psychology and Social Research 200.
Kalindi, S.C. (2006), The impact of the new primary reading programme on the poor readers. University of Zambia. Unpublished M.Ed Dissertation
Katzao, J J. & Likando, G. N. (2010). Educational Reform in Southern Africa – Prospects for the new millennium – The case of Namibia. In Wolhuter, C. C. & Herman, H. D. [Eds]. Educational Reform in Southern Africa – Prospects for the new millennium. Potchefstroom: CC Wolhuter
Kelly, M. J. (2000). Reading comes first. Primary reading programme baseline readingstudy. Lusaka: MOE.
Kotze, H., Higgins, C. and Tabulakani (1999). Breakthrough to Ichibemba pilot project. An evaluation. Lusaka: MoE
Lerkkanen, M.-K. (2003). Learning to Read: Reciprocal Processes and Individual Pathways. Jyväskylä Studies in Education, Psychology and Social Research 203.
Mann, V., & Wimmer, H. (2002). Phoneme awareness and pathways into literacy: A comparison of German and American children. Reading and Writing: An Interdisciplinary Journal, 15, 653–682.
Matafwali, B. (2005). Nature and prevalence of reading difficulties in the third grade: The case of Lusaka. Unpublished MEd dissertation, University of Zambia, Lusaka.
Matafwali, B (2010). The relationship between oral language and early literacy development. A case of English and Zambian languages. University of Zambia: Unpublished PhD Thesis.
Mbenzi, P. A. (1997). Analysis of reading Error patterns of Grade 5 learners at Namutoni Senior Primary School and how to overcome them. Fieldwork Report: University of Namibia, Windhoek.
Ministry of Education. (1993). Toward Education For All. A Development brief for Education, Culture and Training. Windhoek: Gamsberg Macmillan.
Ministry of Education (1996), Educating our Future. Lusaka: ZEPH
Ministry of Education. (2005). Lower Primary Phase Syllabus, English First Language.
Ministry of Education. (2005). Lower Primary Phase Syllabus, English Second Language.
Ministry of Education. (2006). Syllabus for lower primary education grades 1-4 in the BETD. Okahandja: NIED.
Ministry of Education. (2009). Education and Training Sector Improvement Plan (ETSIP). [Online]. Available: http://www.mec.gov.na/ministryOf Education/etsip.htm [2009, June 27].
Nkamba, M. & Kanyika, J. (1998). The Quality of Education: Some policy suggestions Based on a Survey of schools. Zambia. SACMEQ Policy Research: Report No. 5. Paris: ILEP and Lusaka: Ministry of Education.
Nkamba, M. & Kanyika, J. (1998). The Quality of Education: Some policy suggestions Based on a Survey of schools. Zambia. SACMEQ Policy Research: Report No. 5. Paris: ILEP and Lusaka: Ministry of Education
Namibian Languages. http://www.biodiversity.org.na/dbase/NamLanguages.php [2010, March 06].
Ojanen, E. (2007). Sewero la-ma-u-a a phonetic approach to literacy development. Master thesis. Univeristy of Jyväskylä. Department of psychology. http://urn.fi/URN:NBN:fi:jyu-2007702
Poskiparta, E. (2002). Remediation of Reading Difficulties in Grades 1 and 2. Are Cognitive Deficits Only Part of the Story. Annales Universitatis Turkuensis, Serie B, part 254.
Puolakanaho, A., Ahonen, T., Eklund, K., Leppänen, P.H.T., Poikkeus,A-M., Tolvanen, A., Torppa, M.,& Lyytinen, H. (2007). Very early phonological and language skills: estimating individual risk of reading disability. Journal of Child Psychology and Psychiatry,48, 923–931.
Republic of Namibia, (2003). 2001 Population and Housing Census National Report, Basic Analysis with Highlights. Windhoek, National Planning Commission.
SACMEQ. (2004). A study of the conditions of Schooling and the Quality of Primary Education in Namibia. By D. K. Makuwa, National Research Coordinator.
Seymour, P. H., Aro, M., & Erskine, J. M. (2003). Foundation literacy acquisition in European orthographies. British Journal of Psychology, 94, 143–174.
Snow, C.E., Burns, M.S. & Griffin, P (eds.). (1998). Preventing reading difficulties in young children. Washington, DC: National Research Council.
Williams, E. (2004). The screening effects of English in Sub-Saharan Africa. I: Sandøy, Helge et al [Eds] Den fleirspråklege utfordringa. Oslo, Novus Forlag, s. 31–56.
Wikan, G., Mostert, L., Danbolt, A. M. V., Nes, K., Nyathi, F. & Hengari, J. (2007). Reading among grade six learners in Namibia and Norway. An investigation of reading habits and attitudes of learners in the Khomas and Oshana regions of Namibia and the Hedmark region in Norway. Elverum: Høgskolen I Hedmark.
Wimmer, H., & Mayringer, H. (2002). Dysfluent reading in the absence of spelling difficulties: A specific disability in regular orthographies. Journal of Educational Psychology, 94, 272–277.
Publications associated with Graphogame or the research on which it is based
Hintikka, S., Aro, M., & Lyytinen, H. (2005). Computerized training of correspondences between phonological and orthographic units. Written Language and Literacy, 8, 155–178.
Hintikka, S., Landerl, K., Aro, M. & Lyytinen, H. (2008). Training Reading Fluency: Is it important to practice oral articulation and is generalization possible? Annals of Dyslexia, 58, 59–79.
Huemer, S., Aro, M., Landerl, K., & Lyytinen, H. (2010). Repeated reading of syllables among Finnish-speaking children with poor reading skills. Scientific Studies of Reading, 14, 317–340.
Kujala, J., Richardson, U., & Lyytinen, H. (2010). Estimation and visualization of confusability of matrices from adaptive measurement data. Journal of Mathematical Psychology, 54, 196–207.
Kujala, J., Richardson, U., & Lyytinen, H. (2010). A Bayesian-optimal principle for learnerfriendly adaptation in learning games. Journal of Mathematical Psychology, 54, 247–255.
Lyytinen, H. (2010) State-of-Science Review: New Technologies and Interventions for Learning Difficulties: Dyslexia in Finnish as a Case Study. In Cooper, C., J. Field, Goswami, U., & Jenkis, R., B.J. Sahakian (Eds.), Mental Capital and Mental Wellbeing. UK: Office of Science and Innovation. Oxford: Wiley-Blackwell. Pp. 859–866.
Lyytinen, H., Erskine, J., Ahonen, T., Aro, M., Eklund, K., Guttorm, T., Hintikka, S., Hämäläinen, J., Ketonen, R., Laakso, M.-L., Leppänen, P.H.T., Lyytinen, P., Poikkeus, A-M., Puolakanaho, A., Richardson, R., Salmi, P., Tolvanen, A., Torppa, M. & Viholainen, H. (2008). Early identification and prevention of dyslexia: Results from a prospective follow-up study of children at familial risk for dyslexia. In G. Reid, A. Fawcett, F. Manis, & L. Siegel (Eds.), The SAGE Handbook of Dyslexia (pp. 121–146). Sage Publishers.
Lyytinen, H., Erskine, J., Kujala, J., Ojanen, E. & Richardson, U. (2009). In search of a sciencebased application: A learning tool for reading acquisition. Scandinavian Journal of Psychology, 50, 668–675.
Lyytinen, H., Ronimus, M., Alanko, A., Poikkeus, A. & Taanila, M. (2007). Early identification of dyslexia and the use of computer game-based practice to support reading acquisition. Nordic Psychology, 59,109-126.
Ojanen, E., Kujala, J., Richardson, U. (in press). Technology-enhanced literacy learning in Zambia: important observations from a multilingual literacy environment. Language and Education.
Richardson, U., Aro, M. & Lyytinen, H. (in press). Prevention of Reading Difficulties in Highly Transparent Finnish. In P. McCardle (Ed.), Dyslexia Across Languages: Orthography and the Brain-Gene-Behavior Link. Baltimore: Brookes Publishing.
Saine, N. L., Lerkkanen, M.-K., Ahonen, T., Tolvanen, A., & Lyytinen, H. (2010). Predicting word-level reading fluency outcomes in three contrastive groups: Remedial and computerassisted remedial reading intervention, and mainstream instruction. Learning and Individual Differences, 20, 402–414.
Saine, N. L., Lerkkanen, M.-K., Ahonen, T., Tolvanen, A., & Lyytinen, H. (2011). Computer-assisted remedial reading intervention for school beginners at-risk for reading disability. Child Development, 82, 1013–1028.

Tuija Aro, Phanwell Namangala, Pamela February,
Kalima Kalima and Tuire Koponen
4. Mathematics
How are difficulties in learning mathematics manifested?
In Finland, eight-year-old Joel’s parents and teachers were puzzled over his problems in learning mathematics. The teachers were worried about Joel’s extensive difficulties in math, which caused him anxiety studying with the class because the tasks were far too difficult. Addition and subtraction with small numbers were time consuming and Joel resorted to counting with his fingers as he calculated. When pairs of numbers that add up to ten were being practised, Joel knew them fairly well, however, after a week he had forgotten them. Joel lacked confidence in up-over-ten addition. His parents felt that Joel was good at mathematics, if only he wanted to make an effort. They thought Joel’s problems with mathematics had come about because, for some reason, he had started to hate math.
Gift was a pleasant 11-year-old Zambian boy. He did not speak much, but had a good sense of humour and often loved to play with toys. Gift was able to read and enjoyed science subjects. He did not like to do calculations as he found them difficult and time consuming. When he was adding, he required a lot of space because he would use many objects for counting, especially for problems requiring addition and multiplication. Gift was able to count to ten using his fingers. For additions that go beyond 10, rather than continuing to count with his fingers, he wanted to count using his toes as well. For example, to solve “3 x 6” he counted to 10 with his fingers and then removed his shoes to count the numbers above 10 with his toes. His parents and teachers thought that Gift was lazy and often threatened him with punishment for failure to find solutions to math problems.
Mathematical skills consist of several separate skills. In preschool-age, children have an inborn interest in quantities, changes, and words that describe these. In school-age, learning disabilities in mathematics are seen, for example, in calculation errors and in difficulties to learn and retrieve arithmetical combinations (i.e., 4 + 3 = 7) from long-term memory, and instead using counting-based calculation strategies which tend to be prone to mistakes and are difficult for the student to change even with diligent practice. As with dyslexia, the starting point for the diagnosis of a mathematical learning disability is considering whether the child has received sufficient teaching and the difficulties are unexpected compared with the child’s general cognitive performance and age group. Often difficulties are accompanied with the child’s self-concept of being unskilled in maths and having a distaste for it. Difficulties in mathematics often appear together with other learning problems. Additionally, as can also be seen in the African countries, language background poses a problem for children who have to switch from their mother tongue language to English as a medium of instruction when they come to school. For many children in Africa, English is a second or third language. Though math is already in and of itself a difficult subject for many children, they have to learn this complex subject in a “foreign” language that they do not fully master. This tends to ex-acerbate the problem. Furthermore, poor teaching instructions may further contribute to children having problems in learning concepts and skills. This may be due to a teacher’s own poor mathematical knowledge; the teacher may not have received adequate training in mathematics education or may also have a negative attitude towards teaching mathematics. Fundamental mathematical concepts, such as counting, ordering, correspondence, classification and conservation should be taught and the teacher should make sure that learners have internalised these concepts before moving on to formal mathematics.
What causes difficulties in learning mathematics?
Hereditary factors have been found to be behind difficulties in learning mathematics as well, but it is still unclear to what extent and what role heredity plays. Efficient learning of maths requires learning and mastering various skills, and thus it also requires several cognitive functions. Language, spatial, and memory problems can all be seen to be related to problems in learning mathematics. However, research has not yet yielded a clear picture of which mathematical skills different cognitive functions might be connected with. Nonetheless, specific numerical abilities with possible deficiencies can be identified (such as the ability to recognise and judge or compare numerosities between small quantities. In the literature on neuropsychology and developmental neuropsychology, difficulties in mathematics have been associated with extensive syndromes such as the Gerstmann syndrome and Nonverbal Learning Disability (NLD). The main characteristics of the Gerstmann syndrome are difficulties in discriminating the fingers of the hand (finger agnosia), in left-right orientation, and in academic skills relating to mathematics and writing. In NLD, difficulties with tactual and visuospatial perception, mastering of concepts, and applying acquired mechanical skills are in the foreground. With regard to mathematics, the greatest challenges are in mastering the skills that are necessary for applying the number system and solving tasks that are spatially oriented, such as geometry.
From the viewpoint of comorbidity, for example, the simultaneous occurrence of difficulties in language development and learning mathematics is an issue. Particularly counting skills, reciting number-words in the correct order, and understanding relational concepts cause difficulties for preschool-aged children with language disabilities. According to some studies, children with language disabilities do not count numbers while enumerating quantities as their peers do. They tend to be less successful in quantification tasks that amount to over five. At a later age, children with language disabilities have been noted to have deficits in basic calculation skills, which never develop to the fluency of their peers, and in their ability to translate numbers into numerals or vice versa. In a study on children with language disabilities, the most significant distinguishing factor between those fluent in calculation and those who relied on counting based strategies was their ability to retrieve the names of familiar objects and colours quickly from memory (Rapid Naming Test).
Table 11. The early identification of mathematical difficulties at home, school and the psychologist’s assessment
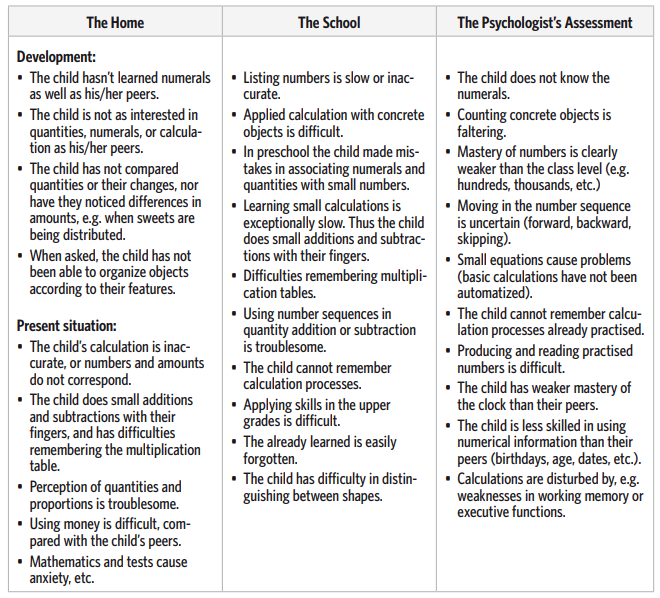
Development of mathematical skills
Mathematical skills can be categorised in many ways. One way is to divide the spectrum of skills roughly into four classes: Counting, number concepts, arithmetic calculation skills, and relational concepts. Counting means the skill to produce numerals in the correct order and to move fluently through number sequences. Quantity perception, which develops quite early, is considered to be a nonlinguistic process that is apparently based on spatial conception and upon which the later understanding of number sequences is developmentally based. Producing numbers and performing demanding calculations require the understanding of number concepts as well as number sequences. Usually the child learns the number sequence first as a rhyme, the individual words of which are given meanings later. To be able to use number sequences in quantity calculation, the child must understand, for example, one-to-one correspondence (each object is counted only once), the cardinality principle (the final listed numeral signifies the quantity of the entire counted set), and the fact that numerals must be listed in a specific order. Mapping out the development of these early skills helps to assess the nature and the degree of difficulty of the possible mathematical learning disability.
For fluency in calculation skills, it is important to know how to use a number sequence in such a way that listing can be begun at any point in the number sequence and any parts of the number sequence can be examined separately. With such skills, it is easy to skip numbers in the sequence (e.g., listing only even numbers, or every fourth number) and to move in different numerical directions. Number sequence skills and number concepts are merged in numeracy, which means the ability to calculate, for example, quantities and changes, and to compare relations between quantities. The child’s calculation strategies develop along with his/her skills. In the development of addition skills, the child first learns enumeration based calculation methods in which the use of the fingers is central. The development of these calculation strategies is affected by, for example, the child’s understanding of the aforementioned principles, the serial nature of number sequences and their quantity, as well as his/her ability to produce numerals. Later, through practice, the child learns more effective and quicker solutions in which the answer is retrieved directly from memory. The learning of more effective strategies is affected by, for example, the development of memory processes. Mastering mathematics also requires understanding several concepts.
Examples of concepts needed at an early stage in life include relational concepts which concern change and that describe relations (e.g., more, larger, behind, later). Learning these seems to be connected with general language development as well. It should be noted, however, that many African languages may not have a description for mathematical concepts and quantities, which may cause additional difficulties in learning mathematics. Some cultures do not have terms for geometrical shapes; for example, the word “triangle” does not exist in most local languages in Namibia. This poses a problem for the learner because he/she has no reference point anchored in his/her background.
Mathematical learning disabilities, the environment, and interaction
Math is a very hierarchical subject by nature: Earlier deficiencies in knowledge and skills affect the assimilation of new matter. If a child has fallen behind the rest of the class in math, catching up can feel hopeless. It is hard for such a child to achieve experiences of success in mathematics, especially when teaching moves on to new contents, as his/her understanding requires a mastery of previously taught matters. As a result, difficulties in mathematics easily raise aversions and feelings of hopelessness towards the whole subject. Because of his/her difficulties in math, the child may also feel more like a poor student in general. This weakens school motivation and the child’s self-concept as a learner may become exceedingly negative. Mathematical skills are also needed in upper grades, in other subjects such as physics for instance, and the ramifications of this should naturally be taken into account when planning support. At the same time, math is also a subject in which some difficulties, such as problems in memorising the multiplication table, are not necessarily connected with other mathematical skills.
This is why the assessment of math skills or know-how cannot succeed if it is based only on individual skills. The child’s math skills must be extensively mapped out to obtain a general impression of his/her skills. From the child’s viewpoint, this means that he or she should not define him- or herself as a poor student of mathematics merely because he or she has difficulty in multiplication for instance, as he/she may be successful in other mathematical areas such as number sequences and understanding the base ten (denary) numeral system at the level of the class. At the onset of the school years, a student may need the help of the teacher or another adult to understand this and keep his/her attitude towards mathematics positive. A point worth remembering is that difficulties in mathematics are solely considered as difficulties in calculation skills, and not in geometry for example.
Assessment of specific skills in mathematics
Learning and mastering the different component skills of mathematics require many kinds of cognitive skills, and thus fluent cooperation between different parts of the brain. The main objectives of a learning disability assessment are to assess:
– understanding of quantities and numbers (such as estimating, comparing, and serial ordering of quantities),
– producing numbers (such as in counting and writing), and
– mastery of basic arithmetical combinations (i.e., numerical facts). In investigating the child’s calculations, a separate assessment can be made of how many arithmetical facts the child has stored in memory (memorised information, such as the multiplication table), how he or she utilises these in calculation (what kind of calculation strategies the child uses), and how well he/she has learned procedures for different methods of calculation (such as borrowing and memory rules). The child’s mistakes should be examined closely. The psychologist or teacher can specify whether the child makes mistakes in regard to place values, numbers, borrowing, storing to memory, basic knowledge, calculations, or symbols. The examination of these factors requires a solid understanding of the development of mathematical skills and the progress of teaching. From the viewpoint of practical work, the consideration of difficulties can be simplified with rough subtypes. For example, Geary’s subtypes help us discern in which functions the child’s difficulties primarily seem to be. He specifies three types of difficulty. The first is the so-called semantic memory difficulty, in which it is difficult for the child to learn mathematical facts and he/she makes mistakes when trying to retrieve them from memory. The second is the so-called procedural difficulty, in which it is difficult for the child to remember principles and rules for calculations; for example, difficulties in understanding number concepts may be involved. In the third subtype, visuospatial difficulties are emphasised; the child finds it hard to organise and handle numerical information spatially and might make mistakes placing numbers one above the other.
In the following table, mathematical skills have been classified by synthesising different theories. The assessment column describes tasks and tests with which each specific skill can be assessed. References to tests can be found at the end of the chapter.
Table 12.Assessment of mathematical skills

Basil, 1985), and Spiers’ (1987) classification of mathematical errors.
Table 13. ICD-10 Classification of specific mathematical disorders
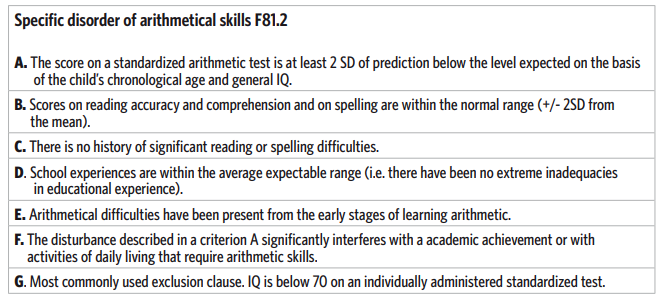
References
Geary, D. C. (1993). Mathematical disabilities: Cognitive, neuropsychological, and genetic components. Psychological Bulletin, 114, 345–362.
Koponen, T., Mononen, R., Räsänen, P., & Ahonen, T. (2006). Basic numeracy in children with specific language impairment: Heterogeneity and connections to language. Journal of Speech and Hearing Research, 49, 1–16.
McCloskeyn, M., Caramazzan, A., & Basilin, A. (1985). Cognitive mechanisms in number processing and calculation: Evidence from dyscalculia. Brain and Cognition, 4, 171–196.
Spiers P. A. (1987). Acalculia revisited: Current issues. In G. Deloche & X. Seron (Eds.) Mathematical Disabilities. A Cognitive Neurospychological Perspective. Hillside NJ: Lawrence Erlbaum.
BANUCA – Basic numerical and calculation abilities
Räsänen, P. & Maslov, O. (in preparation). BANUCA –Basic numerical and calculation abilities. The test and the manual. Jyväskylä: Niilo Mäki Institute. [in Russian and Unkranian]
Räsänen, P. (in press). BANUCA –Basic numerical and calculation abilities. The test and the manual. Jyväskylä: Niilo Mäki Institute. [in Somali]
Räsänen, P. & Bulto, N. (in press). BANUCA –Basic numerical and calculation abilities. The test and the manual –Ethiopian localized version. Addis Ababa: Ministry of Education. [in Afan Oromo]
Räsänen, P. & Bulto, N. (in press). BANUCA –Basic numerical and calculation abilities. The test and the manual –Ethiopian localized version. Addis Ababa: Ministry of Education. [in Amharic]
Räsänen, P. (2005). Banuca – lukukäsitteen ja laskutaidon testi luokille 1–3. Jyväskylä: Niilo Mäki Institute. [Basic numerical and calculation abilities: a test for grades 1–3][In Finnish]
Räsänen, P., & Chilala, M. (2003). BANUCA –Basic numerical and calculation abilities. The test and the manual. Lusaka: Zambian Ministry of Education. [In English]
Räsänen, P., & Chilala, M. (2003). BANUCA –Mutomo wa Kukona Kubala ni Kusebeza Lipalo. Lusaka: Zambian Ministry of Education. [In Silozi]
Räsänen, P., & Chilala, M. (2003). BANUCA –Kuwerengera ndi Kulemba Manambala Koyamba. Lusaka: Zambian Ministry of Education. [In Cinyanja].
Räsänen, P., & Chilala, M. (2003). BANUCA –Lweeseko lwa jiibuumba. Lusaka: Zambian Ministry of Education. [In Kiikaonde]
Räsänen, P., & Chilala, M. (2003). BANUCA –Manambala atachi nañovu Zhakuzata. Lusaka: Zambian Ministry of Education. [In Lunda]
Räsänen, P., & Chilala, M. (2003). BANUCA –Musunko Wakuzyiba a Kubeleka Nsamuzi. Lusaka: Zambian Ministry of Education. [In Chitonga]
Räsänen, P., & Chilala, M. (2003). BANUCA –Ukubelenga amanambala nookupenda. Lusaka: Zambian Ministry of Education. [In Icibemba]
Räsänen, P., & Chilala, M. (2003). BANUCA –Vyseseko Vyalizavu. Lusaka: Zambian Ministry of Education. [In Luvale)
Tuija Aro, Mwiya. L. Imasiku, Cynthy Haihambo, Andrew Möwes,
David Kariuki and Timo Ahonen
5. Attention and executive functions
In Finland, the parents and teachers of nine-year-old Jonas discussed the difficulties he was having at school. In the classroom Jonas was restless and had problems controlling his emotions. Jonas could handle most tasks as well as his classmates, as long as he could first contain himself enough to begin them. Spelling was the only subject that Jonas had real difficulties with. Writing was toilsome for him and he made many mistakes. It was strenuous for Jonas to hear phonemes, and erasing mistakes felt repulsive. His father reported occasional critical situations at home because of Jonas’ fits of rage and restlessness. Sometimes Jonas did his homework quickly and easily, but there were often arguments about when he should do it. On other occasions, homework took a lot of time. Playing with friends drew Jonas’ attention away from homework. The teacher had also observed that Jonas had friends at school and playing during breaks was important to him. But he had friction with a few friends, especially during afternoons, and often an adult was needed to help calm things down.
In Kenya, Njeri’s father sought help from the Kenyatta University Clinic because he could not cope any more with the state of his two daughters. He did not come with the girls to the first session. He indicated that Njeri was 7 years old while her sister was 5 years old. In brief, he explained that his daughters were too hyperactive, both at home and school, to the point of becoming a nuisance. He insisted that the assessor visits the home after the girls come home from school. On the appointed day, the assessor did visit the home and found the father alone at the house – the girls were out playing in the neighbourhood. A casual observation of the house indicated signs of seats that had been ripped open by the girls, and toys and other paraphernalia were scattered all over the place. A guided visit to the girls’ bedroom revealed more. There were footprints on the ceiling above the children’s double-decker bed. The girls came in soon afterwards and it was clear that they were extremely hyperactive. Due to the well-defined referral request, diagnostic assessment was performed on both girls and the results confirmed severe Attention Deficit Hyperactivity Disorder. In the typical classroom in Namibia, the most frequent types of unwanted behaviour problems reported by teachers are children talking out of turn and hampering other children. Other behaviour problems, such as lying, stealing, truancy, fighting, fire-setting and vandalism were not mentioned so frequently as these took place outside the classroom and thus very seldom disrupted the work of the class. Behaviour patterns that were preventing the teacher from teaching were related to attention-seeking and disruption. A child with severe difficulties in behaviour regulation often behaves like he or she has no respect towards other people, neither for the teacher nor the system, and sometimes peers do not show respect to the problematic child and may think bad of him or her. From the students’ point of view, a lack of motivation and boredom were major problems.
These problems can be related to a fear of failure and can later on result in behaviour such as disruption and attention-seeking. Children with behavioural problems may also suffer from low self-esteem and a diminished sense of self-worth. They may think of themselves, “Since I am useless and perceived by others to be useless and hateful, then I might as well behave as I like and live up to that image”.
There are many reasons why learners have emotional, social and/or behavioural difficulties. Low self esteem and lack of motivation can be barriers to learning. One of the causes is deprivation; other causes may be Attention Deficit Hyperactivity Disorder (ADHD), or simply attention-deficit, where the learners may daydream or forget what they are doing (Brown, 2005). Recent research data collected from the South African primary school teachers (Perold, Louw, & Kleynhans, 2010) shows that their overall knowledge of ADHD is still poor. For instance, in Zambia many teachers are ignorant of the ADHD conditions of their pupils and students. Therefore they end up punishing such children instead of helping them to manage their affliction. Parents of children with ADHD often have very negative experiences to report. Among other things, parents’ main concerns include their own lack of understanding ADHD and the general lack of knowledge and skills regarding the best suited ways of supporting children with ADHD through action plans. Admittedly, what makes the situation worse is the fact that even the health care professionals from whom they expect help lack understanding of the ADHD condition. Therefore, parents are thrust into a kind of feeling of being in the dark and having to cope without support or information. Going by the Zambian educational policy of inclusive education, it is clear to see that most parents want their children to stay in mainstream schools, but they also realise that mainstream teachers are often too busy and pressurised to cope.
The main characteristics of attention-deficit disorders are inattention (difficulty in focusing and maintaining attention on essential things; lack of concentration), hyperactivity (fidgeting and other movement inappropriate for the situation), and impulsivity (acting quickly without considering consequences). These are described (see Table 16) by the diagnostic criteria for Attention Deficit Hyperactivity Disorder (ADHD) and Hyperactivity Disorder, set out in official psychological classifications. For example, the child may fidget or run around in inappropriate situations, he or she may fall deep into thought or seem distant, or be too hasty or rash in his or her actions. In many cases, difficulties in working independently (beginning or completing a task) or planning actions may be symptoms of an attention deficit disorder. In disorder assessment the child’s activity is compared with that of their peers in similar situations. To meet the diagnostic criteria of ADHD, the characteristic behaviour must have been observed already before school-age and in several different situations (e.g., at school and at home), meaning that it must be the child’s typical way of acting and reacting in different situations. ADHD can manifest itself in completely different symptoms, so that inattention may be the sole symptom in one child, while another child may only express motor hyperactivity, and a third may have both symptoms. The child’s behaviour may not always meet all the criteria but can still be so disturbing that the child needs special support in order to accomplish crucial development tasks and establish peaceful study conditions in the classroom, as well as to ensure the well-being of the family. Thus, the fulfilment of diagnostic criteria or a doctor’s diagnosis must not be too predominant when deciding whether the child needs more or different support from adults.
ADHD is diagnosed according to the child’s behaviour. Nevertheless, cognitive difficulties often accompany the disorder. These difficulties do not necessarily appear in the child’s test performance. A definite connection between cognitive performance and behavioural characteristics cannot be drawn. However, based on research literature, it can be said that attention problems are often related to problems with executive functions, or children’s difficulties in planning their own functioning, performing tasks systematically and evaluating their own performance and results. Problems with executive functions often manifest themselves as difficulties in tasks that require consideration and weighing of alternatives, but they may also appear as more subtle difficulties such as in the child’s inability to organise his or her own activity, especially in new or complicated situations and duties. Thus, some of the central objects of assessment are the child’s ability to work independently, to plan his or her own activity, to begin and complete tasks, and to make an effort.
Table 14.How problems with attention appear at home, at school, and in the psychologist’s assessment
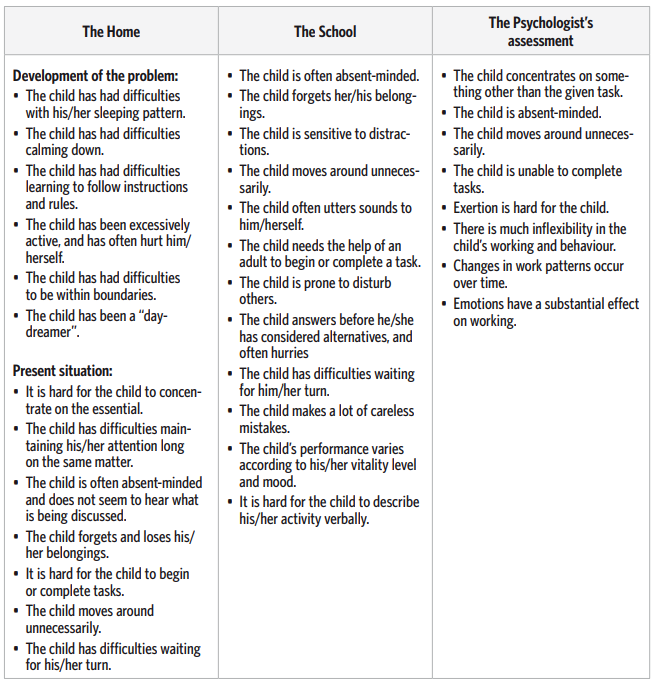
Attention can also be approached cognitively through its different elements. In such a case, the assessor examines factors like the child’s ability to focus their attention on what is essential and to maintain his or her attention on the subject matter in spite of distractions, and also to alternate his/ her attention between different matters flexibly and controlled. These component skills of attention can to some extent be assessed with separate tests (see Table 15). Often low self-esteem and difficulties in behaviour and learning accompany attention-deficit disorders. Especially difficulties in learning to read are typical of children with attention-deficit disorders. According to some studies, especially those children whose attention problems are mainly related to inattentiveness run a greater risk of meeting with learning problems. However, these results were achieved by studying groups rather than individual children. Also, an attention deficit disorder does not necessarily coincide with other difficulties.
What causes attention deficit disorders and difficulties in executive functions?
The causes for attention deficit disorders are not fully understood yet, but heredity is known to be a key factor (Tripp & Wickens, 2009). Apparently, the child’s hereditary tendencies, together with the environment and its interactional relationships, affect the way and extent to which the child’s difficulties manifest themselves in daily life. The disorder is known to have a neurological basis, even though it is diagnosed based on the child’s behaviour. In particular, the neurotransmitters of the brain have been actively studied. Children with attention deficit disorders are known to have abnormal functioning of these neurotransmitters. Much neurological and neuropsychological research has been performed on the frontal and parietal lobes which are known to be involved in attention and self-regulation. In addition to ADHD, some neurological illnesses or learning disability types manifest difficulties with executive functions. Difficulties with executive functions are typical in connection with language development problems and visual difficulties, and also when the child has the Nonverbal Learning Disability (NLD) which is often accompanied by visuo-spatial and social difficulties. Children that were prenatally exposed to alcohol (FAS or FAE) often also manifest difficulties with executive functions and behavioural characteristics typical of ADHD.
Difficulties with executive functions are often mentioned in connection with Tourette’s syndrome, and they are known to surface especially when coinciding with ADHD. Adequate executive functions require the ability to observe one’s activity as if from outside oneself and to have an awareness of one’s functioning in general (the so-called Theory of Mind). A deficiently developed Theory of Mind is often connected with autistic symptoms and the Asperger’s syndrome, which may partially explain why difficulties with executive functions are often observed with these disorders. Difficulties with executive functions are also frequently observed in connection with depression and brain damage, especially when the damage is in the frontal lobe of the brain.
Development of attention and executive functions
Problems in attention and behaviour regulation appear when the demands of the environment increase, as is often the case at school. To understand the difficulties and define their causes, it is good for the assessor to know about the child’s earlier development as well. Even according to the definition of ADHD, the child must have had signs of the difficulty before school-age. The developmental starting points of controlling one’s own activity and behaviour are in the baby’s inborn desire to control him/herself and his or her ability to anticipate events and consistencies in the environment. With these skills, children begin to build their conception of events in their environment and the consequences of their actions. The fact that children know they can understand and anticipate events in their environment, and that they affect themselves and the environment, is the basis for the development of each child’s self-regulation. If the environment offers the child consistency, sensitivity to their initiatives, encouragement and boundaries as they learn new things, this strengthens the child’s self-conception as an individual able to affect events and his or her own activity. When a child succeeds in a task that requires self-regulation, he or she will try to regulate his/her activity even more in the future. Experiences of success also help the child overcome frustrations. Even in later stages of development, as well as in support, the consistency of the environment and successful experiences of self-regulation are vital.
During the second year of their lives, children become aware of social demands. They can commence, maintain, and discontinue actions according to social expectations and comply with requests from adults. Around their second birthday, the child can wait and delay a requested action and regulate his or her activity according to social expectations, even without external guidance. Usually around the third year, the child has a fair ability to take changing circumstances into consideration and to adapt his or her activity according to the different demands of the environment. Thus, difficulties adapting their own actions to given instructions or demands of situations may be signs of a difficulty in behaviour regulation, and therefore indications for intervention planning. Accumulating cognitive skills, such as language and memory, are central and support the development of behaviour in regard to self-regulation. With age, children direct their activity more and more according to verbal instructions. They also increasingly self regulate their activity by speaking of events out loud.
At first they describe events after they have occurred, but gradually (inner) talk that is addressed to themselves, or private speech, begins to precede events (i.e., thinking before speaking or doing). By then the child has realised that he or she can affect events with language and thus his/her own and other people’s actions. In connection with attention-deficit disorders, it has been noted that the activity directing private speech of children with ADHD who are under school-age is more often focused on irrelevant issues than that of their peers. This supports the assumption that there is a link between speech and successful executive functions. Some children have difficulties following verbal instructions. They need much repetition in order to learn rules and to comply with social demands. In addition, they often need more concrete feedback than their peers in order to learn that some patterns of activity are not allowed or that these patterns are not good for them. Such children often act impulsively with no prior thought regarding the consequences, and thus they often break the boundaries set by adults. Continuous defiance may be a sign of the child’s difficulty in internalising rules and following verbal instructions. Impatience in waiting for wishes to be met changes with age, but if the child still has evident difficulties at the age of five, then it may be a sign of difficulties with self-regulation.
Research on the cognitive development of attention has revealed that an infant already observes stimuli from the environment, but the events and stimuli of the environment direct his or her attention. As the child develops, he/she can more actively focus his or her attention on stimuli that are meaningful for the situation or task. The ability to plan and organise activity appropriately for the objective also develops with age. These skills are often discussed under the concept of executive functions. The years from the age of six onward are a time of intense development in general, but also specifically in the child’s ability to maintain and inhibit motor functions and to understand series and orders that have to do with time. The child’s ability to plan things beforehand, to consider alternatives and the different perspectives on things, and to set goals for his or her own actions, develop strongly during the first school years. Furthermore, development in these skills still continues significantly even in the individual’s second decade.
Difficulties with attention and executive functions, the environment and interaction
Emotional difficulties often accompany deficit disorders; for example, low self-esteem, depression and anxiety occur more often among children with attention problems than their peers. Even if none of these rather serious mental problems are noted in connection with an attention deficit disorder, there is reason to pay special attention to the child’s interactive relationship with the environment. A hyperactive or impulsive child often ends up defying shared rules or boundaries set by adults, and is thus regularly in conflict with his or her environment. Such a child requires exceptional consistency and patience from their environment, both at home and school. The child’s parents and teachers may feel exhausted and powerless with the child. If the adult involved with the child is tired or unsure, then he or she cannot always be consistent or sensitive enough to the child’s needs, or may not be able to support the child’s growth or development of self-esteem. A cycle of negative interaction often forms between the adult and the child, which increases the problems further and affects not only the child’s self-concept, but also the adult’s faith in his or her own ability to be an educator or parent. In such a case everyone involved needs help, that is, in addition to the child’s development, the adult must also be supported.
A child with an attention deficit disorder cannot always understand why it is harder for him or her to act according to the wishes of adults or their friends, or why they are unable to complete tasks independently while their peers can. Recurrent failure in tasks or friendships easily leads to an overly negative self concept. This, for its part, has a detrimental effect on the further development of the child’s self-image. Thus it would be beneficial for the child if his/her difficulties were detected as early as possible, so that forms of support that help the child cope with his or her environment in daily life can be found before the problems escalate. At school, a child with an attention deficit disorder benefits if the teaching and all other functions consist of as much repetition of unchanging practices and methods as possible and plenty of instructions that support the proper focusing of attention (Daly, Creed, Xanthopoulos, & Brown, 2007; Young & Amarasinghe, 2010). In addition, removing all excess stimuli from tasks, the teacher’s actions, and the daily routine and classroom is helpful for many children, especially those who have problems paying attention (see below).
Box 4. An example from Namibian experience
Before the child’s behaviour reaches the stage of becoming disruptive, the teacher can engage the child in some activity that the child likes and enjoys, and praises the child for performing well. The teacher can even draw up a chart where the child’s good behaviour is being reflected and decide on a specific reward system. The teacher can decide together with the child what rewards would suit both of them. Behaviour modification is a powerful technique which can be used successfully in the classroom to manage problematic behaviour. Drawing up a contract with the child is another positive structured way of eliminating problematic behaviour and to get the child’s cooperation. The child now agrees to behave in certain ways and to carry out certain obligations, such as being on time for lessons, while the teacher agrees to fulfil his or her part in return. The teacher will then make a note on the personal contract sheet each time the child has met a particular requirement that was discussed. The contract sheet accompanies the child the whole day. At the end of the day or the end of the week, progress is monitored and any necessary changes are made to the initial agreement. A reward system can also be considered, which links up with behaviour modification strategies.
Assessment of attention and executive functions
An ADHD diagnosis is based on the child’s behaviour in different situations. Thus, the child’s parents and other adults who know the child are vital for assessment. For a successful assessment to take place, it is important to obtain information on the child’s activity in both one-to-one and group situations, for example, with regard to questionnaires and interviews. Frequently children operate differently in strange situations than in familiar situations. In the assessment, it is sometimes necessary to study the child longer than the customary 45 minutes (e.g., 3 x 45 minutes), to see how the child’s or adolescent’s ability to function and exert him/herself changes with time or fatigue.
Information from the parents about their child’s early stages helps to assess the difficulties in the long run. This is important for assessing the extent of the difficulties and their prognosis as well as for the purpose of being able to make a differential diagnosis. Information on the child’s development helps to assess whether his or her problem primarily concerns attention or is, even partially, the child’s way of reacting to a frightening or anxiety-causing life situation, for instance. Parents can also explain the methods used in the family to overcome the problems and provide an overview of their daily life. Aspects to be examined in one-to-one assessments should include:
• motor restlessness,
• the ability to focus attention on essential things,
• the ability to maintain attention long enough on essential issues,
• changes in attention during the course of the assessment,
• sensitivity to external stimuli and distractions,
• straying from the task or topic of discussion,
• getting stuck on, for example, a certain action, stage, or topic of discussion,
• impulsivity,
• changes in alertness, and
• difficulties exerting oneself.
The term “attention” is also frequently used to refer to the cognitive dimensions of attention, which can sometimes be confusing. Even though it is used to refer to both behaviour and cognitive skills, the two concepts mean quite different things. The connection between attention on the behavioural level and cognitive factors in and of themselves is not unambiguous. Children with an attention-deficit disorder often perform according to their age level in neuropsychological tests meant for attention assessment. In other words, the requirements of tasks planned for attention assessment do not always uncover a child’s difficulty. In addition, a child may be given plenty of encouragement and support in the assessment situation, which together with short and interesting tasks helps him or her to work more attentively than usual. From a cognitive point of view, attention is seen to consist of several different subfunctions, for example, the ability to focus attention on essential issues, maintain attention on the subject matter, flexibly change the object of attention or pattern of activity, and to consider several things simultaneously (see Table 15). Deficits in these subfunctions may appear in many tests. A deficiency in skills is often rather seen in the child’s way of carrying out a task (e.g., straying, getting stuck, and lack of planning) than in the final score.
Cognitive tasks that reveal the child’s problems cannot be unambiguously named based on existing research literature, even though, for example, tests for assessing executive functions have been developed. However, especially tests that require planning, effort and perseverance are undoubtedly sensitive to attention-deficit disorders. Such tests may include memory tasks, tasks given a time limit, and tasks that require maintaining activity or considering more than one issue at a time. Skill necessary for successful executive functions are, for example, the ability to set goals, to plan activity, and to complete the task whilst considering the demands of the situation. Table 15 describes the cognitive components of attention common to most theories and provides examples of psychological tests and daily situations in which difficulties with each component in question can occur. References relating to tests can be found at the end of the chapter. Table 15 (the lower part) also describes the most central stages of executive functions and the difficulties observed in each one.
Table 15. Assessment of the component functions of attention and executive functions

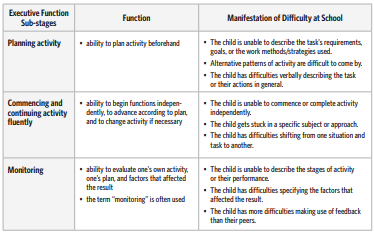
Table 16. Diagnostic criteria for Attention-Deficit/Hyperactivity Disorder ADHD, DSM-IV
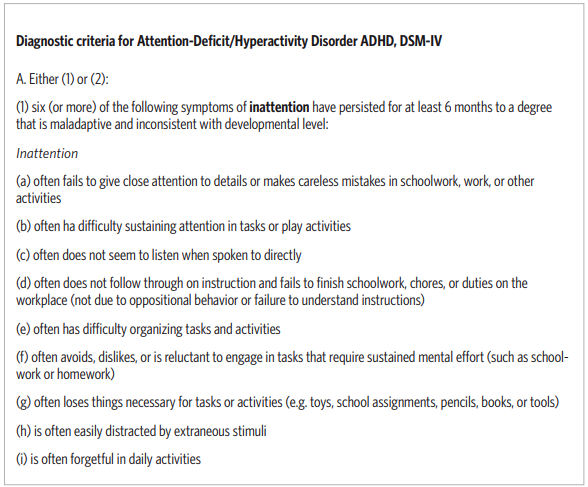
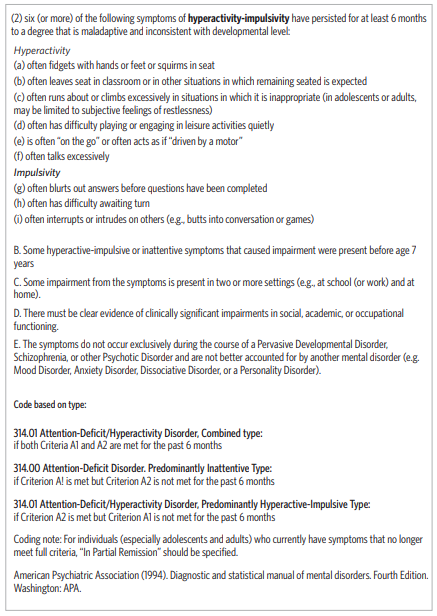
References
Brown, T. E. (2005). Attention Deficit Disorder. The Unfocused Mind in Children and Adults. New Haven: Yale University Press.
Daly, B.P., Creed, T., Xanthopoulos, M., & Brown, R.T. (2007). Psychosocial treatments for children with attention deficit/hyperactivity disorder. Neuropsychological Review, 17, 73–89.
Heaton, R.K, Chelune, G.J., Talley, J.L. et al. (1993). Wisconsin Card Sorting Test. Manual. Odessa, FL: Psycyhological Assessment Resources.
Janols, L-O., Kadesjö, B., Korkman, M., Michelsson, K., Strand, G., & Trillingsgaard, A. (1998). A Nordic Questionnaire of a Child’s Development and Behavior.
Kadesjö, B. (2001). “Five to fifteen” – A Nordic Questionnaire of a Child’s Development and Behavior. In K. Michelsson & S. Stenman (Eds.), The Many Faces of Attention-Deficit/Hyperactivity Disorder (pp. 124-134). Helsinki: Signe and Anne Gyllenberg Foundation.
Perold, M., Louw, C., & Kleynhans, S. (2010). Primary school teachers’ knowledge and misperceptions of attention deficit hyperactivity disorder (ADHD). South African Journal of Education, 30, 457–473.
Reitan, R.M. (1971). Trail Making Test results for normal and brain damaged children. Perceptual and Motor Skills, 33, 575–581.
Tripp, G. & Wickens, J.R. (2009). Neurobiology of ADHD. Neuropharmacology, 57, 579–589.
Waber, D.P. & Holmes, J. M. (1985). Assessing children’s copy productions of the Rey-Osterrieth Complex Figures. Journal of Clinical and Experimental Neuropsychology, 7, 264–280.
Young, S. & Amarasinghe, J.M. (2010). Practioner’s review: Non-pharmacological treatments for ADHD: A lifespan approach. Child Psychology and Psychiatry, 51, 116–133.

Tuija Aro, Phanwell Namangala, Sophie Kasonde-Ngandu,
Beatrice Matafwali and Timo Ahonen
6. Language functions
How are difficulties in language development manifested?
Peter was a Finnish boy whose language development had been slow and he was given speech therapy before school-age. His vocabulary accumulated slowly, and for a long time his speech was inarticulate. Peter used pronouns in place of nouns and would sometimes also use self-invented words. It was always difficult for him to narrate events. At school he had received remedial instruction in mathematics and special education in his mother tongue since the first grade. Now, in the third grade, he encountered difficulties in English (as a second language) and in history. It was difficult for Peter to understand instructions given to the whole class. He found making sense of texts troublesome and frequently needed the help of an adult. Peter could not do his homework independently, so it was agreed at home that he would do his homework when his parents came home from work. Schoolwork took so long and was so difficult for him that the special education teacher suggested individualised teaching. In the negotiation with the school, it was decided that they would have a psychologist assess the extent of the necessary individualisation of the teaching.
Five-year-old Chanda from Zambia could not speak from an early age. At the age of 18 months, his parents became concerned and sought expert advice. He was diagnosed with anklyloglossia, a condition commonly known as tongue-tie. He underwent surgery at the age of two years and was immediately put on speech therapy in which the preschool and the mother were actively involved. The programme was evaluated every six months over a period of two years by a speech therapist. This intervention yielded positive outcomes as evidenced by a remarkable improvement in Chanda’s speech. However, when he started first grade at the age of seven, his teacher observed some gaps in Chanda’s language articulation that were unusual for his age group and he was subsequently immediately referred for further assessment.
Chanda’s articulation problems were confirmed and it was noted that also his receptive language was not developed according to age expectations. Difficulties in language development are roughly divided into problems with understanding and those affecting production (see Table 19). However, in order to be able to plan effective support, it is necessary to assess the nature of the language disorder more precisely. The phenotypes of language disorders can be examined in more detail, for example, with the help of theoretical models or subgroup taxonomies based on clinical observations. Several subgroup classifications have been devised relating to language disorders, of which the commonly used taxonomy devised by Rapin and Allen is presented at the end of this chapter (see Table 20).
An estimated 3-7 percent of the population has problems concerning language development (Tomblin et al., 1997). Diagnostic names used are: specific language impairment (SLI), developmental language disorder, and specific developmental disorder of speech and language (see ICD-10). These indicate that a child’s language develops clearly more slowly than his or her other developmental skills, and that this is not due to a hearing impairment or neurological illness, nor as a result of mental retardation. Learning disability assessment may reveal language difficulties that are more moderate or limited than actual language disorders that would also affect the child’s learning and social interactions. Signs of a difficulty in language comprehension that are milder than actual dysphasia may be
• difficulties acting according to given instructions,
• requests to repeat instructions, or
• difficulties in reading comprehension. Signs of problems in language production may be
• reluctance or difficulties with verbal self-expression,
• lack of expressions,
• difficulties finding words, or
• replacing words by paraphrasing or with pronouns (see Table 17 for more details).
Even moderate language difficulties should be taken into consideration in making a learning disability assessment and planning support. Deficits in language skills may coincide with difficulties in learning mathematics, literacy, foreign languages, reading comprehension, and sometimes with social behavioural problems as well. If the difficulties are considerable, the child should be referred for further assessment in order to be diagnosed appropriately and to receive the proper benefits and services. Furthermore, the earlier stages of the child’s language development and the possible language development characteristics of the family should be tracked, for example, by interviewing the parents.
Table 17. The manifestation of moderate developmental language disorders at home, at school, and in the assessment situation
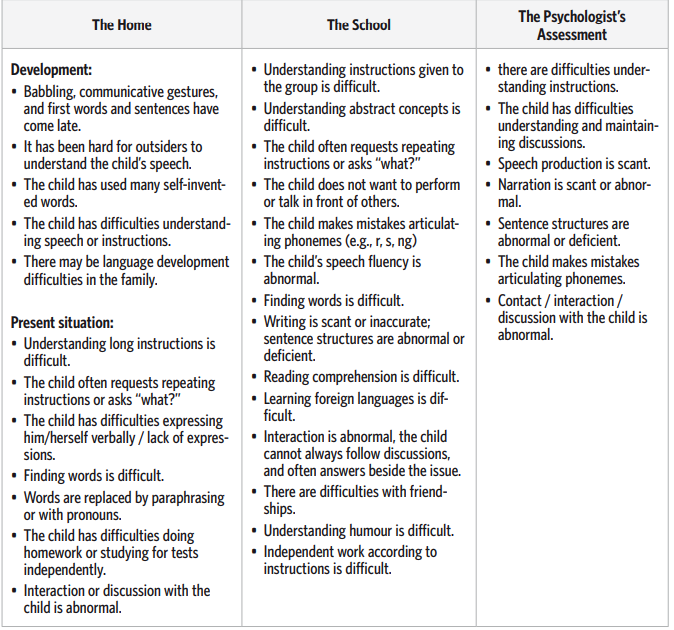
What causes language disorders?
When the causes of language difficulties are examined, several factors arise on many levels. As with other difficulties, one of the significant objects of research in language disorders has been heredity. It is assumed that hereditary factors affect the development of the central nervous system, causing functional or structural changes in the parts of the brain that are central for producing and understanding language. These changes predispose the child to language development problems. Even though the mechanisms are not yet known, the role of heredity in language disorders is indisputable. However, it is important to remember that some of the children with language disorders have no relatives that suffer from similar difficulties. In addition to heredity, causes for language disorders have been sought in early nervous system development and environmental factors. For example, light weight at birth, premature birth, or an especially low APGAR score all have been associated with language development problems in school-age.
Some syndromes are also accompanied by language difficulties. Even though environmental factors cannot explain language disorders, the social environment plays an important role in supporting the child’s language development. With this in mind, the environment’s language and possible supportive actions for language development should be assessed when support is planned for the child.
Language development
Information on delayed development in language production or comprehension is considered to be important when making an assessment of a child’s language skills. Parents can often describe the main characteristics of their child’s language development, but the assessor must know how to ask defining questions and be sensitive to clues of a possible difficulty in language development as he or she listens to the parents’ narration. Interaction with adults and other children is important for the development of language skills.
Adults’ sensitivity to the child’s messages, their ability to adapt their speech according to the child’s skills and to enrich these as the child grows, all support the child’s language development. From the early stages on, language development is linked to the environment, and the language spoken in the environment affects which phonemes and phoneme combinations the child is sensitised to, and which are strengthened as the child utters sounds. Phoneme development is quickest during the first and second years of in life, and begins with the child producing vowels. Then, at approximately seven months of age, the child begins to produce consonant-vowel syllable series. In the early stages of language development, deviations are natural, but a three-year-old already knows all of the vowels of his or her mother tongue. Flawless consonant production can be expected at 4 or 5 years of age. In their early years, children understand more language than they can produce, which they demonstrate by communicating with gestures and facial expressions as well as by following given instructions. It is important to monitor the development of understanding speech, especially when word production is believed to be delayed. If it is hard for the child to understand brief instructions and he/she does not use words, then his or her language development must be monitored more closely than if he/she does not produce words but understands speech. Rapid accumulation of vocabulary begins at about 1½ years of age, when the child masters about 30-50 words.
At around the third year of age, the child should produce words from several word classes, which should be taken into consideration when making an assessment, in addition to vocabulary size. During the second year in life, the child begins to combine words. The first word combinations are expressed in a telegram style and do not follow grammar. However, development is rapid and a three-year-old already masters several different types of sentences, and by five years of age a child’s speech normally contains all of the primary language’s types of main and subordinate clauses. Once the first word combinations have been produced, the child very quickly learns inflections as well. Development is quickest at 2-4 years of age, and a five-year-old already masters the basic rules linked to inflections. Misapplying rules or making mistakes with unusual words are still natural at this point. If a 5- or 6-year-old child still uses many incorrect inflections or self-invented words, then his/her language development should be examined more closely and possible support options should be considered. Normally, a five-year-old can tell a short story consistently, and a six-year-old can already describe the significant details as well.
Narrative skills have been noted to predict the child’s future school success, which is why their assessment should be included in the child’s language development assessment. Sometimes a child’s language difficulties have to do with a deficiency in his or her ability to use language as a tool for social interaction. Unfortunately, such problems often go unnoticed before the onset of schooling. In some cases, these characteristics have been observed earlier but the child has only been considered “a bit special”, or his/her difficulties have been interpreted from the viewpoint of interaction rather than deficient language development. In school-age, when the demands of social skills grow and interactive relationships become more diversified, difficulties in using language for interaction become more evident. Sometimes only detailed assessment reveal that the problem is connected with language development as well.
Developmental language disorder or normal variation?
Epidemiological studies have shown huge individual variation in the age at which children first begin to speak. This variation is comparable with the significant variation in reaching other developmental milestones, such as walking independently and reaching puberty. Of the markedly late talkers at the age of 2 to 3 years, about half appear to have caught up by the age of five (Rescorla, 2005), and of these most continue to show normal language performance, though some may show subtle deficits. A disorder, rather than normal variation, is likely if
• the child’s babble is impaired in quantity or abnormal in quality,
• there is limited use of babble for social communication,
• the understanding of language is limited,
• there is little attention paid to other people’s talk,
• there is little communicative use of gestures,
• there is poorly developed pretend-play,
• there is a family history of definite language problems,
• if socio-emotional functioning is impaired, and/or
• there are problems in motor control as indicated by marked drooling, problems in chewing, and/or problems in blowing.
If none of these areas show abnormalities, then the probability (but not certainty) is that the issue may be nothing more than a normal variation in language acquisition. If any or all of these indicators show problems, some form of disorder would need to be considered and further assessment is needed (Rutter, 2008).
Difficulties in language development, the social environment, and interaction
Language is the instrument of thought and interaction. With language, the child organizes his or her emotions, environment and self. Language development difficulties affect the child’s overall development in many ways. The ability to express oneself and to share experiences with others in one’s social environment is necessary for the development of the self. When a child encounters language difficulties, ways to support communication development, such as with gestures, should be sought as early on as possible. The consequences of only moderate language difficulties for the development of the child and his or her interactive relationships are, naturally, less severe, reminding us that early intervention is all the more important in the more serious cases. Language disorders that go unobserved until school-age are often so mild that their impact only affects the learning of school subjects. For example, moderate language difficulties may be behind difficulties in learning to read or reading comprehension. Verifying these in an assessment helps the child and also makes it easier for his/her social environment to understand the child’s difficulties in learning and to support him or her.
Sometimes even moderate language development problems present themselves as difficulties in self expression. For instance, difficulties in producing sentences or finding words may hinder speech to the extent that the child has problems communicating with his or her peers, particularly during or approaching adolescence. Public performing or writing compositions may also feel difficult, uncomfortable, or cause anxiety. Even moderate comprehension difficulties may impede the child’s learning because, for instance, in a noisy classroom it is hard to follow instructions given to the whole class, especially if they consist of long sentences. In such a case, the child needs teaching that is as explicit and concrete as possible. Language difficulties in which it is hard for the child to use language as an instrument for social interaction, naturally, involve social problems as well. The child may be quite clumsy in situations involving interaction; they may not be able to direct their speech at others or to advance the discussion reciprocally whilst taking their friends’ initiatives into consideration. They may also be too blunt, which becomes a problem especially if it causes the child or youth to get into conflicts or makes them feel left out or lonely. Some language disorders and learning disabilities are accompanied by difficulties in understanding figures of speech or humour and in combining what is said with the nonverbal communication. Such a difficulty may hinder forming social relationships and make the child feel like an outsider and lonely, especially on the threshold of puberty.
Assessment of language functions
The assessment of language skills takes place on several different levels: Tests, interviews, questionnaires, and observations. During assessment, it is important to listen to the child’s spontaneous speech and the possible phoneme and grammatical mistakes, or difficulties in finding words. Also when assessing narrative skills, it is good to note the child’s spontaneous speech when, for example, telling about pictures. In this way, the amount of detail and consistency of the narrative, as well as the child’s ability to consider the listener, can be assessed. In discussion with the child, the assessor must pay attention to the reciprocity of the child’s speech, in addition to the aforementioned factors. Discussions in assessment situations are formal, and the child’s speech is often scant or only given in response to the adult’s initiatives in these situations. Therefore it is good to assess language skills and their early development with questionnaires or by interviewing the people who are close to the child. Temple (1997) offers a simplified model of handling language information as a basis for assessment. The starting point of the model is that processing language information requires unimpaired auditory perception. This is followed by phonological analysis, or the processing of the parts of a word. Difficulties at this stage of the process may appear as, for instance, difficulties in discerning the exact phonemic structure of the word. In the assessment situation, this may be seen in problems such as the child repeating words that are difficult or new to him or her.
Inaccurate whole words in the child’s speech may be a sign of difficulties on this level. When a word is heard and processed, the word’s meaning (semantics) is activated. In an assessment, semantic difficulties can appear as scant vocabulary, problems understanding concepts, and/or toilsome or inaccurate retrieval of words (word finding or naming difficulty). If the child has used a lot of self-invented words, facial expressions, gestures or paraphrasing in the earlier stages of his or her development, or if he/she has learned new words slowly, then the possibility of a semantic deficiency should be assessed. The vocabulary of a child with a language disorder is often narrow, but it can also be irregularly developed so that he or she may for instance have surprising mastery over concepts in one area, but in another area there are clear indications of a conceptualising difficulty. The narrow vocabulary of children with language disorders is thought to be due to, for example, difficulties in perceiving and remembering the exact phonological forms of words (as mentioned earlier). A child’s learning of new words by utilising general knowledge of language may also be deficient, slowing down vocabulary development.
In school-age, a mild semantic difficulty can present itself as problems in understanding ambiguous words or expressions, and as difficulties using and learning new concepts. This can then impede, for example, reading comprehension. Word finding and naming difficulties may show up in daily speech in the form of excessive use of paraphrasing or pronouns and pauses in speech. In an assessment situation, such a difficulty manifests itself particularly in naming and rapid naming tasks, but also in other tasks during which the child may, for instance, point at the right answer instead of saying it. Especially, difficulties in rapid naming are often associated with difficulties in learning to read, but they have also been noted to have a connection with other learning disabilities (e.g., mathematics). Syntax means combining words so that they form meaningful entities that follow grammatical rules. For sentences to be correctly formed, words must be inflected – this is called morphology. Language difficulties on this level appear as grammatical mistakes, wrong inflections or scant sentence forms. The slow development of sentence forming or the prolonged use of telegram-style speech may be developmental signs of this difficulty. In school-age, inflection mistakes are rare in moderate language difficulties. The difficulty may be seen in, for example, occasional mistakes in case inflections in speech or in writing compositions.
For a person to produce speech, they must be able to programme and control their speech muscles precisely. Problems on this level manifest themselves as oral or verbal dyspraxia, and may first occur developmentally as a delay in beginning to babble and utter words. Later on the child’s speech may contain syllables or phonemes in the wrong order (catcus = cactus, ephelant = elephant), or be marked by abnormal emphases, or prosody. In Table 18, the aforementioned model of language functions has been complemented with a description of pragmatic skills. Sub-processes have been proportioned according to the tests generally used by psychologists and speech therapists. In addition, the last column describes how difficulties with each sub-process manifest themselves in daily life and schoolwork. References relating to the tests can be found at the end of the chapter.
Peter’s story continues, showing how developmental language disorders quite often appear at school-age together with other learning difficulties such as in reading and/or mathematics. A discussion with the school psychologist revealed that Peter’s mother’s pregnancy had progressed without problems until week 36, when she suffered toxaemia, which led to the forced induction of his birth. Peter’s weight at birth was 2,250 kg. In regard to his motor development, Peter’s parents said that he had learned to sit without support at 10 months and to walk at 15 months of age. He spoke his first words just before being two years of age, and his first two- and three-word sentences shortly before turning three years old. After this, his vocabulary accumulated slowly and especially outsiders found it difficult to understand Peter’s speech. He made many phoneme mistakes. His parents reported that he had learned motor skills (e.g., cycling and skiing) almost on a par with his peers. At the child health clinic and day care centre they were worried about Peter’s development, so he started speech therapy at four years of age in order to increase his vocabulary and improve his narrative skills.
The parents said that Peter was generally a happy and active boy. He had plenty of friends. At home, during the third grade, they began having heated quarrels about homework. Peter needed help with many tasks and it often took him several hours to complete them. In spite of the difficulties, Peter went to school readily. His mother said that she herself had also had difficulties in school, especially with learning to read and foreign languages. She recalled having to work very hard at it, and still her performance had not been very good. A questionnaire for the teachers revealed that the main problems hindering Peter’s schoolwork were his difficulties in understanding task instructions and written texts, and his slow reading. He also had deficiencies in understanding individual words in texts. Decoding was slow but flawless. Verbal tasks in mathematics were difficult and Peter needed much time for basic calculations. Peter was a diligent student and he worked hard on tasks, but he had difficulties understanding collectively given instructions. Hence, he followed what others did and imitated them. Peter had many friends and he was socially active. During the psychologist’s assessment, Peter worked well and concentrated well. For the most part, Peter’s performance was slightly below his age level in tasks that assessed his general skill level. His nonverbal performance was clearly stronger than his language performance. Peter did not have deficits in his executive functions, which would have explained many of his school difficulties. He had evident difficulties in tasks that assessed verbal concepts, word finding, verbal memory, understanding of language, or perception and production of phonemic structures. Peter’s mastery of inflections was on a par with his age group. His visual perception, fine motor skills and nonverbal problem-solving skills were also as proficient as was typical for his age. Naming letters, and syllable- and word-level reading, were slower compared to his age group, and reading comprehension was considerably difficult for him. His spelling skills were below the level of his class. When Peter’s mathematical skills were assessed, he did well in calculating small additions and subtractions when he had ample time. Calculations with larger numbers were difficult because Peter had deficiencies in his mastery of the base-ten numeral system. His number sequence skills were poor and he found applied mathematical tasks considerably difficult.
Table 18. Assessment of language functions
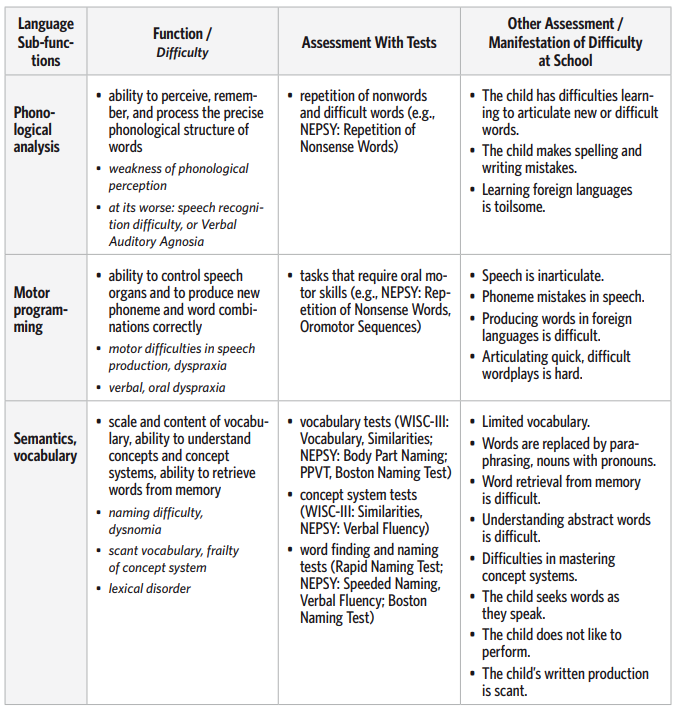
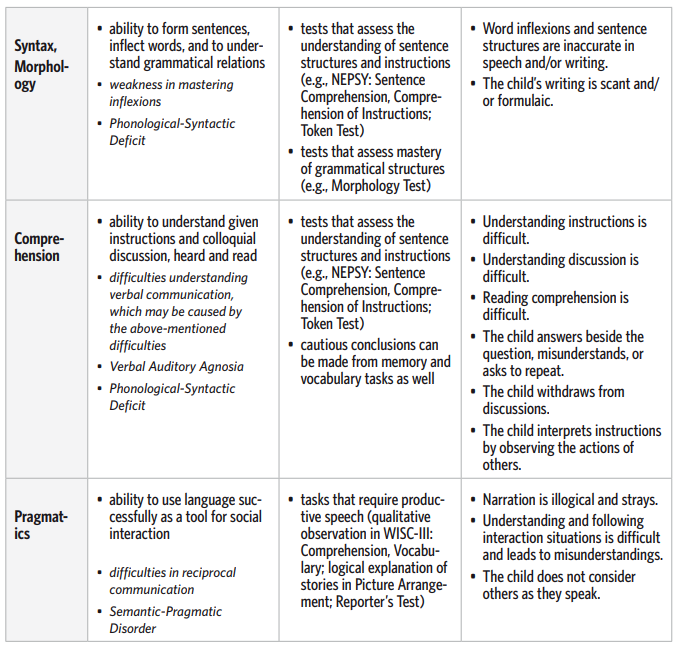
Table 19. Diagnostic criteria of Specific developmental disorder of speech and language

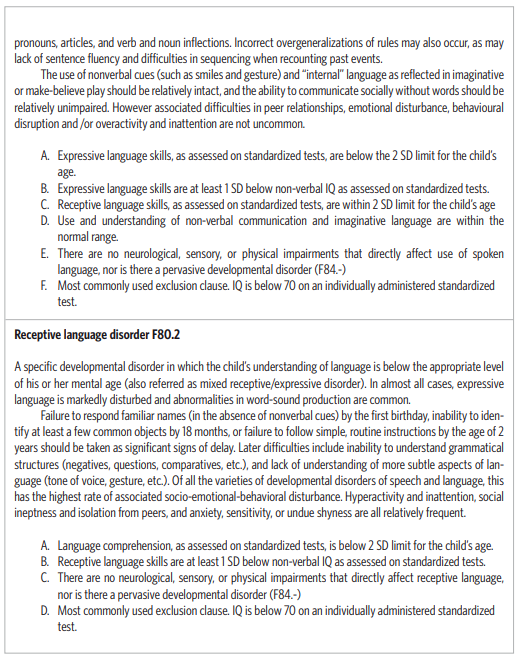
Table 20. Subgroups according to Rapin and Allen (ICD-10)
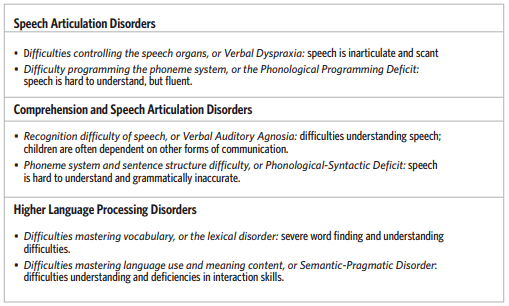
References
De Renzi, E. & Faglioni, P. (1978). Normative data and screening power of a shortened version of the Token Test. Cortex, 14, 14-49.
De Renzi, E. & Ferrari, C. (1978). The Reporter’s Test: A sensitive test to detect expressive disturbances in aphasics. Cortex, 14, 279-293.
DeRenzi, E. & Faglioni, P. (1978). Normative data and screening power of a shortened version of the Token Test. Cortex, 14, 14-49.
Dunn, L.M. & Dunn, E.S. (1981). Peabody Picture Vocabulary Test –Revised. Circle Pines, MN: American Guidance Service.
Kaplan, E.F. & Goodglass, H. (1983). The Boston Naming Test. Philadelphia: Lea & Febiger. Rapin, I. & Allen, D.A. (1983). Developmental language disorders: Nosologic considerations.
In Kirk, U. (Eds.), Neuropsychology of Language, Reading, and Spelling. New York: Academic Press.
Rescorla, L. (2005). Age 13 language and reading outcomes in late-talking toddlers. Journal of Speech and Hearing Research, 48, 459–472. Rutter, C.M. (2008). Diagnostic concepts and risk processes. In C.F. Norby, J.B. Tomblin, & D.V.M. Bishop (Eds.), Understanding Developmental Language Disorders (pp.205–215).
East Sussex: Psychology Press.
Temple, C.M. (1997). Cognitive neuropsychology and it’s application to children. Journal of Child Psychology and Psychiatry, 38, 27–52.
Temple, C.M. (1997). Developmental Cognitive Neuropsychology. Hove, East Sussex: Erlbaum.
Tomblin, J.B., Records, N.L., Buckwalter, P., Zhang, X., Smith, E., & O’Brien, M. (1997). Prevalence of specific language impairment in kindergarten children. Journal of Speech and Hearing Research, 40, 1245–1260.
Tuija Aro, Cynthy Haihambo, Daniel Muindi and Inonge Ndalamei
7. Visual, visuospatial and
visuoconstructive skills
How are visual difficulties manifested?
In Finland, in consultations held at eight-year-old Hanna’s school, Hanna, her parents, the class teacher and the special education teacher were present. The teachers had discussed the learning difficulties Hanna had in mathematics and her mother tongue, and her possible need of a psychologist’s assessment. The class teacher said that Hanna needed much individualised support. At school her performance varied – sometimes things went fine and sometimes they were a real struggle. Her mother said that they had noticed the fluctuation of her performance at home as well. They could not estimate her time spent on homework because sometimes she did them quickly and at other times similar tasks might take even a few hours. The parents had noticed that Hanna’s behaviour had differed greatly from that of her big brother, already before school-age. She had always been a shy and timid girl. She tried to secure situations long beforehand. It took her a long time to make friends, and especially to get acquainted with new adults. Hanna could not remember where things were at home and her parents had to help her pack her schoolbag because she had difficulties following her timetable and packing her bag accordingly. The teachers said that Hanna had the most problems in mathematics. She had trouble keeping a number in mind as she calculated. Subtractions were especially difficult. Counting from twenty to one was troublesome. In her mother tongue she had difficulties with writing. She reversed letters and numbers, and her use of pencils was slow and a bit clumsy. In physical education, the teacher had noted Hanna’s difficulty with spatial perception. For example, in team games Hanna had problems placing herself and moving around the field. It looked like Hanna retreated to the side of the field and was afraid of the ball.
Ben, a boy from Zambia, was 9 years old in grade 3. It was observed that while in grade 2, Ben used to isolate himself from others and was overly dependent on others, as well as lagging in activities in daily living. He followed a slower development course in the acquisition of daily skills such as eating, lavatory use and dressing. When it came to reading in class, his friends used to laugh at him because he used to shed tears when reading, and he would repeat words and his eyes blinked excessively. He was also very slow when it came to the copying of work. He would omit letters and parts of the work. This worried the teacher who decided to approach the parents. The mother remembered that Ben suffered from measles and cerebral malaria when he was five years old. She said this could be the reason Ben had these problems that affected his learning. This led to an agreement that the child is to be taken to the eye specialist for an assessment of the problems with his eyes. It was felt that the information from the doctor would also be useful for the educational psychologist in planning intervention. The doctor discovered that Ben was myopic, or shortsighted, and prescribed some correctional glasses. After correcting his eyesight, Ben’s performance and self-esteem improved and helped him to work despite his other difficulties.
Henry, from Kenya, was a grade 5 pupil who always selected the desk in the last row at the back of the class. His schoolwork was often untidy and had many mistakes, and he was frequently punished for not completing his work on time. When prompted to answer a question by the teacher, he frequently kept quiet although the teacher felt that he could try a little harder. During one test, Henry was caught looking at a colleague’s answer booklet. During games, Henry was frequently mocked by his play-mates because of his poor performance. His parents and teachers were concerned because they could see the boy’s self esteem dropping as time went on. Henry was referred for help at Kenyatta University’s Neuropsychology Clinic, where a simple eye assessment test using the Snellen chart revealed shortsightedness. A referral was made to an ophthalmologist who confirmed compromised visual acuity. It was found necessary for Henry to use large print and shift his seating position in class to the front of the classroom. This case study reveals why Henry wrote in a messy manner, copied from colleagues, gave wrong answers to questions written on the board and missed the ball on the playing field. That is to say, Henry’s problems were caused by poor eyesight rather than visuospatial perception problems. This reminds us that an “eyesight test” should not be ignored, especially in areas where visual acuity is not routinely assessed.
Difficulties with visuospatial perception are often mentioned in descriptions of the child’s development before school-age. The simpler term “perceptual difficulties” is often used, when children are reluctant to do puzzles or cannot dress themselves as well as their peers, or if they frequently put their shoes on the wrong feet. Such children may also find it hard to learn to use scissors or to draw as well as their peers. They may also avoid new places, bicycling, climbing frames, threading a needle or using a mobile phone with small fonts, to name just a few examples. Serious developmental problems with visuospatial perception may present themselves, for instance, as difficulties in copying simple figures or remembering routes, causing the child to frequently get lost even in familiar places. Moderate visual difficulties of school-age children, on the other hand, are not always observed in daily activities. For instance, difficulties with tasks that demand eye-hand coordination (e.g., in handicrafts or art), spatial perception problems (e.g., placing oneself on the field in ball games), or difficulties or reluctance to interpret and utilise visual information (e.g., maps and charts) may be signs of such moderate difficulties. Often the difficulties do not surface until the psychologist’s assessment. The psychologist must perform several tests to find out which functional deficit is behind the child’s poor performance in the assessment situation. Is it a difficulty in visual perception, visuospatial perception or visuoconstructive skills, executive functioning, or in motor functions?
Children’s developmental visual difficulties usually appear extensively in different areas of visuospatial perception or visuoconstruction. In other words, there may be simultaneous difficulties in visuomotor and visuoconstructive skills, and in perceiving visual details or spatial proportions, and in applying this information. Difficulties that are clearly delimited to one subarea of a visual function are usually only seen in connection with brain trauma.
Visuospatial perception is seen to be essential for early quantity perception, and thus for forming numeral concepts, even though otherwise mathematical skills are seen to be strongly connected with language. Difficulties with visual perception are also associated with social perception problems. For example, the child may have difficulties perceiving and interpreting people’s nonverbal messages, such as gestures and facial expressions, or in understanding the social meanings of situating oneself. Furthermore, difficulties in executive functions and in learning concepts, as well as in cause-effect relationships, may sometimes be linked to visual perception difficulties (cf., for example, nonverbal learning disabilities).
Table 21. Visual perceptual difficulties at home, at school, and in the psychologist’s assessment
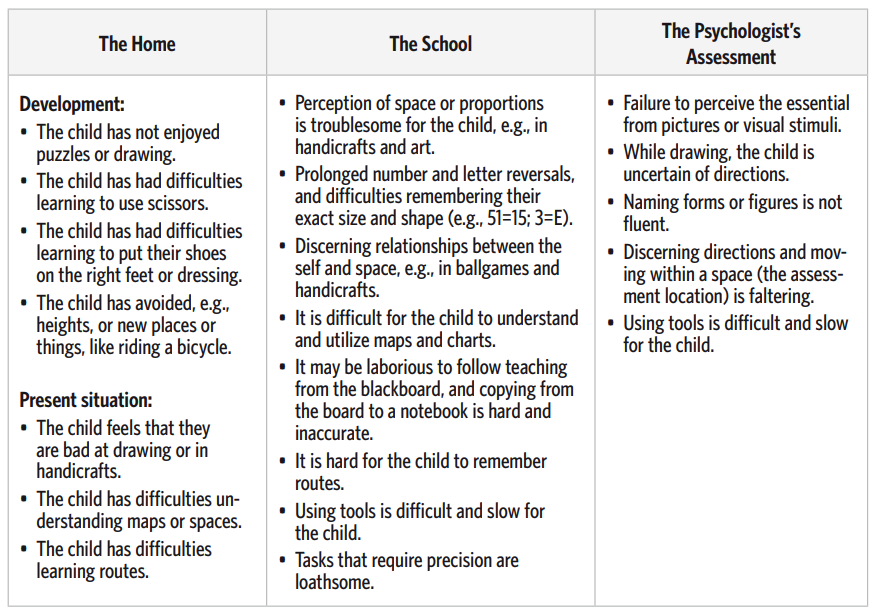
What causes visual difficulties?
The development of visual skills is not as well understood as, for example, the stages of language development and factors that affect it, even though, on the other hand, the neuroanatomy of visual perception is quite well known because of different animal models. Sometimes difficulties are revealed when the child’s skills are assessed in concern over a learning disability. In such cases, the psychologist must often consider what might cause the difficulties observed in daily life and what their connection is with the visuospatial and visuoconstructive difficulties observed in the tests. The psychologist must also often determine to what extent the observed difficulties are deficits in visual perception or visuospatial, visuomotor or visuoconstructive functions, and to what extent they may be due to inexperience or, for example, deficient executive functions. Sometimes assessment may be hindered by the child’s general slowness that causes low performance in time-limited tasks.
Successful visual functions and their integration with other functions require the cooperation of several brain lobes. Successful identification of an object and acting according to the observation requires, in addition to visuospatial perceptions, their fluent association with, for example, memory, motor and executive functions. The actual processing of visual information requires several brain areas. To summarise and simplify the matter, it can be said that the occipital lobe processes visual details and design background differences, the temporal lobe identifies objects and shapes, and the parietal lobe integrates information and discerns directions and proportions. In addition, the mechanisms of the frontal parts of the brain are needed, for example, to inhibit impulses and to plan, organise, implement and evaluate activity. Disorders in each of these areas are likely to affect the success of visual information processing as a whole. Because visual information processing is very complex, and in practice it is linked with, for example, the child’s motor performance, it is understandable that the causes of visual difficulties observed in connection with learning disabilities are not often uncovered.
The root cause of more serious visuospatial difficulties may be early brain damage (CP, premature birth, damage caused by encephalitis, meningitis, or other brain damage), a development disorder of the brain, or a genetic or chromosome anomaly (e.g., Turner-syndrome; XO). Visual difficulties are involved with many other syndromes as well. For instance, prenatal alcohol exposure (FAS or FAE) may lead to many problems, including visuospatial perception and visuoconstructive difficulties. In learning disability assessment, visual difficulties often appear in connection with the so-called nonverbal learning disability (NLD). This difficulty, which is seen as a subgroup of learning disabilities, presents itself in school-age as, for example, visuoconstructive and tactual perception problems and difficulties with memory, processing complex information, and understanding causeeffect relationships, as well as in deficient problem-solving and social skills. The most troublesome school subjects are reading comprehension and verbal and applied tasks in mathematics.
Development of visual skills
Visual skills develop rapidly during the first year of life. They include, for example, visual acuity, depth perception, movement detection and object recognition. Much less is known about later development and the knowledge we do have of it is less precise than the respective knowledge of language development.
The development of visual skills is often assessed through activities such as drawing, even though it is only one kind of task requiring visual skills. Drawing and other visual skills develop and manifest themselves under linguistic control. The child’s ability to linguistically plan their drawing or contructing affects the result. It is also affected by the child’s ability to classify the model and its parts in terms of language. On this basis, some researchers believe that after the early stages in life, visual skills are strongly linked with the child’s other cognitive development and, in particular, with the child’s ability to classify what they see and do verbally. How the child names and controls his or her perception affects what he/she perceives. Language also controls production and thus affects visuoconstruction.
Based on brain damage, we know that the right hemisphere of the brain is active in many stages of visual information processing, such as in form recognition and perceiving directions. However, many spatial perception functions require the left hemisphere as well. Developmentally, the specialisation of the brain hemispheres, or lateralisation, has been observed as early as a few months into the child’s life, but flexibility can also be seen in the brain’s later development, especially in connection with brain damage, when the left hemisphere has been noted to take control of visual skills when necessary. At around the age of ten years, a developmental change takes place: Some visuospatial functions, such as the comprehension of spatial shapes and maps, develop and begin to lateralise.
Difficulties in visual skills, the visual environment, and interaction
If visual difficulties are moderate, they do not distinctly affect the child’s general activity or behaviour frequently. Moderate visual difficulties may easily be dismissed as part of the child’s variety of personal skills. Difficulties using a pencil and orientation problems in the visual environment are often a problem in the early stages of school, when the child must learn to perceive increasingly subtle differences in the environment (e.g., right-left, mirrored numbers 6 and 9) and to relate with the environment in a new way, for example, while walking amidst traffic. More extensive and severe difficulties, for their part, may seriously impede the child’s social activity or their benefiting from teaching. If the variety of difficulties includes difficulties in planning and organising activity, then these may manifest themselves broadly across the child’s schoolwork. Because independent work and homework are toilsome, the need for help may be great. These difficulties are naturally emphasised as school years pass and the demands for independent work increase. If the child has felt inadequate ever since preschool age, it will also affect their self-perception as a student at school. The accumulation of such difficulties can be avoided, for example, by reducing the amount of copying from the board and other notebook work, or by leaving out handwriting, if these are felt to be too overwhelming.
If social skill difficulties are involved with visual difficulties, the child may withdraw and feel lonely and different from the other children. Such a child may find it hard to understand why he or she cannot make friends, why the others don’t like him/her, and why he/she doesn’t understand what the others talk about. In this case, the child needs much help from adults to find his/her place in the class and community of friends. Visual difficulties (especially when nonverbal learning disability is in question) are often accompanied by difficulties in discerning or understanding concepts or cause-effect relationships. This can impede reading comprehension and understanding new conceptual entities. The child may feel stupid because understanding things and succeeding in tests demand more effort from him/her than from his or her classmates. In such a case, practising and applying effective reading strategies is central.
Assessment of visuospatial and visuoconstructive functions
Visual skill assessment is based on both tests and daily observations of functional difficulties. A simplified model helps understand what kinds of substages visual information processing consists of. When a person makes a visual perception, the information from the eye is first processed on the occipital lobe. Here, for example, the stimulus is separated from the background. The cells of the occipital lobe are specialised in processing the angles and positions of the stimulus. From here on information processing continues with two evidently separate processes. The task of the first process, which takes place mainly in the temporal lobe, is to analyse, for example, the shape, colour and structure of the stimulus, and thus to identify the stimulus. This is the ventral (or “what”) route. The task of the second process is spatial perception, or discerning location, direction and size. This is the dorsal (or “where”) route. A person can control their motor activity on the basis of the information that these processing routes gather in the brain. This is necessary for the spatial observation and incorporation of information that is required in, for example, drawing and simple construction tasks. This can be simplified by saying that visual information processing takes place in three relatively independent brain areas: The occipital lobe processes visual details and design-background differences, the temporal lobe identifies objects and shapes, and the parietal lobe integrates information and discerns directions and proportions. In addition, the mechanisms of the front parts of the brain are needed, for example, to inhibit impulses and to plan, organise, implement and evaluate activity.
Successful visual functions thus require cooperation between several areas of the brain, and disorders in different areas have various effects on, for instance, visuomotor performance. Assessing these functions should be included in the child’s assessment in order to understand what it is in the child’s visual information processing that is not working as well as in his or her peers. Table 22 describes the central visual and spatial sub processes, integrating several theories. The assessment column describes which tests generally used by psychologists might reveal a deficit in the function in question, and how it might manifest in daily life. References to tests can be found at the end of the chapter. Individuals who experience problems with the processing of visuospatial information are often faced with serious difficulty in dealing with social and interpersonal situations. Poorly developed interpersonal skills frequently accompany such adaptive deficits. It is therefore very important to make an accurate and early assessment of visual perception.
Table 22. Assessment of visual, visuospatial and visuoconstructive functions
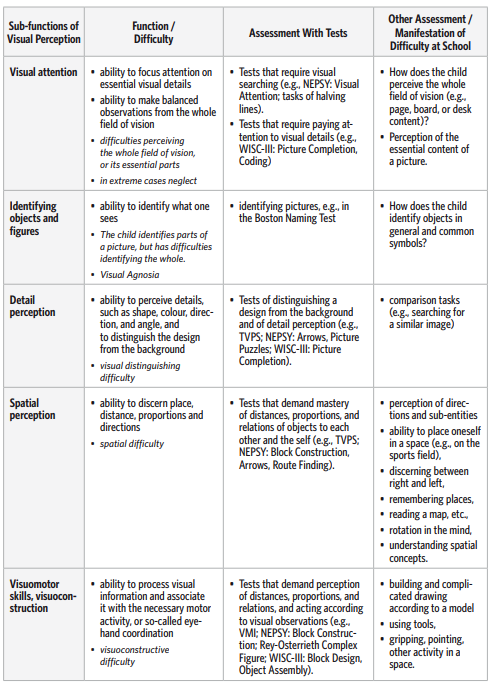
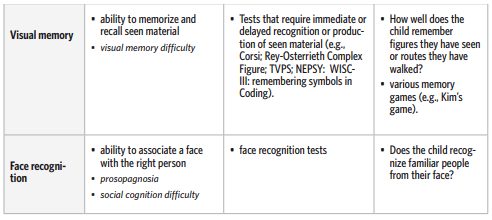
References
Beery, K. E. (1997). Beery-Buktenica Developmental Test of Visual Perception and Motor Cordination
(4th edition, revised). Administration, Scoring and Teaching Manual. Parsippany, NJ: Modern
Curriculum Press.
Corsi’s block-tapping test see M.D. Lezak (1995). Neuropsychological Assessment. (p. 490).
New York: Oxford University Press.
Dijk K., Keeffe J. and Nottle H. (2002). Low Vision Training Manual for Use in Developing Countries.
Cera: East Melbourne.
Gardner, M. F. (1982). TVPS – Test of Visual Perceptual Skills (non motor). Seattle, Washington:
Special Child Publications.
Kaplan, E.F. & Goodglass, H. (1983). The Boston Naming Test. Philadelphia: Lea & Febiger.
Raven, J.C. (1965). Guide to Using the Coloured Progressive Matrices. London: H.K.
Waber, D. P. & Holmes, J. M. (1985). Assessing children’s copy productions of the Rey-Osterrieth
Complex Figures. Journal of Clinical and Experimental Neuropsychology, 7, 264–280.
Further information, see also:
Keeffe, J. (2002) Assessment of Functional Vision Book 2.: World Health Organisation.
Timo Ahonen, Philomena Ndambuki, Douglas Gawani Phiri
and Osman Miyanji
8. Motor skills
How are motor difficulties manifested?
Susan is a seven-year-old girl living in Kenya, attending the second grade in school. When she was five years of age, she was recommended for developmental assessment with the following referral questions. (1) She was unable to display routine motor sequences like throwing objects to a distance of at least three feet (ca. one meter), constructing block towers, and placing an object on a precise spot as per directions given. (2) She displayed an inability to draw geometric shapes, solve simple mazes, or even to reproduce simple designs from memory. (3) She was unable to imitate gestures and actions of others. However, these problems have reduced considerably over the last two years. Nonetheless, the parents felt it would be of benefit to find an explanation for these problems. This was a case of developmental delay, where the stages of motor skill development were delayed but the child was eventually able to make progress to the point of their realization.
Kaunda is a seven-year-old boy from Zambia. He is in grade one at the Kamwala basic school. Within the first two months of Kaunda’s joining the school, the teacher noticed that the boy had difficulties in drawing and writing. Kaunda had untidy handwriting, dropped books, knocked over objects in the classroom and had difficulties in taking part in games like football and running. Having poor motor coordination, he was seen as clumsy and his classmates mocked him. These problems affected Kaunda’s learning ability.
The teacher realized that Kaunda had a problem and he summoned the parents to Kaunda for further questioning about his early childhood. The parents admitted that Kaunda was delayed in the stages of his motor skill development, as he did not walk until he was two years old and had difficulties to dress, tie his shoe laces and feed himself. The mother also said that he was slower than his two older siblings when they were the same age. The mother also remembers that she had a difficult labor and that Kaunda did not cry immediately after birth. The teacher recommended that the parents should consult a doctor, who then confirmed upon assessment that the boy probably had a mild cerebral palsy. Kaunda was finally referred for appropriate therapy and within six months his motor functions and coordination improved and he was a happy boy who could now join his friends in play.
As seen in the examples of Susan and Kaunda, there is individual variation in motor skills, which is apparent in children’s balance-, movement-, and object handling skills. When the child’s motor skills and their development fail – with no clear neurological or muscular reason detected – to meet the environment’s demands to the extent that it causes problems in daily life and impedes the child’s learning and interaction with others, it can be called a motor development disorder, a motor learning disability, or a coordination disorder. In colloquial language it is often said that such a child is “clumsy.”
The official DSM-IV and ICD-10 classification systems describe developmental motor difficulties in a very similar way, even though they use slightly different terminology. What the DSMclassification calls “developmental coordination disorder (DCD),” the ICD-classification refers to as “specific developmental disorder of motor function.” According to the DSM-IV classification, the central symptom of a developmental coordination disorder is an evident difficulty, when compared with the ability and intelligence typical at this age, in functions that demand coordination. This can present itself as slow motor development (e.g., delayed learning to walk, dropping objects, poor handwriting, general clumsiness, or difficulties in sport activities such as running, or throwing and catching a ball). These difficulties appear in regular school performance and hinder everyday life, but they are not caused by a known physical illness (e.g., CP, hemiplegia, or muscular dystrophy). DSM-IV emphasizes assessment of the hindrances to daily life caused by the motor problem, while ICD emphasizes the use of standardized tests for diagnosis.
In spite of the differing emphasis in defining the problem, researchers are quite unanimous regarding their manifestation. Based on studies performed in several different countries, an estimated 6–8 percent of children show some degree of clumsiness, and around 2–5 percent exhibit more serious clumsiness which clearly impedes their activity. These figures reveal that the problem is quite common and not necessarily restricted to movement and manual skills. For school-aged children, clumsiness may also have psychological consequences that affect, for example, the child’s self-esteem and self-image.
As part of a Finnish study (Ahonen et.al., 2004) in a screening of five-year-old children who were also more closely tested at age seven, nearly half of the children were assessed as being clumsy and clearly still had weaker skills than the normal control group in further follow-ups at ages of eleven, fifteen, and seventeen years. These observations are highly consistent with the results of other smaller scale studies. Based on these observations, we can assume that the image created by earlier studies, suggesting a natural spontaneous recovery from mild and moderate motor difficulties, has been too optimistic.
Motor development disorders can occur on their own, but often they overlap with other learning and development disorders. According to several (Visser, 2003) developmental motor disorders are evident especially in connection with attention-deficit disorders and language learning disabilities.
Table 23. The manifestation of developmental motor difficulties at home, at school, and in assessment
situations.
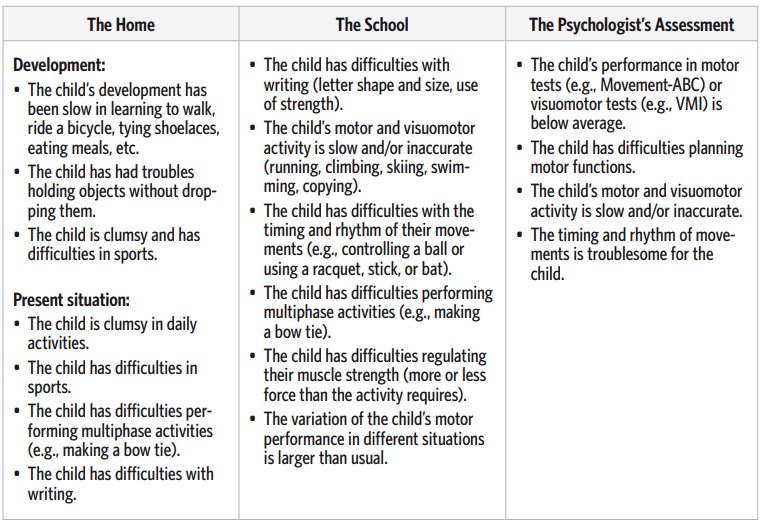
What causes motor difficulties?
No root cause has been clearly identified for development disorders in motor skills. This is understandable as the regulation of motor skills is performed by a large number of structures located in anatomically different parts of the brain and because learning and the environment mould our motor functions constantly. Motor skills are the sum of our nervous system structures and activities which are also influenced by our experiences (Wilson, 2005).
In developmentally clumsy children, signs of precisely located brain damage have not been found, at least not to this day. However, in the few imaging studies that have been performed, about one-third of so called clumsy children have had some kind of structural nervous system abnormality. Nonetheless, the research has not been able to pinpoint a clear connection between the brain structure findings and motor performance. Natal risk factors, such as lack of oxygen, or hypoxia, are relatively common in the developmental history of these children. It is also evident that hereditary factors are equally significant in developmental motor disorders as in other developmental disorders. However, thus far the observations have been based on rather limited research material and clinical discoveries. Studies that focus particularly on the heredity of coordination disorders are still scarce. Several different studies have revealed a connection between kinaesthetic difficulties (identifying body parts and positions without visual observation) and motor performance. Kinaesthetic problems observed in children as early as 4–5 years of age seem to be related to later motor disorders. There are also studies on the relationship between visual difficulties and clumsiness. To compare the performances of developmentally clumsy and normal children, the studies have most often used discrimination tasks involving line-length, size-, shape-, angle-, and size-constancy.
Some studies suggest that the difficulties might pertain more to visuospatial memory and memory retention of positions or movements than to the accuracy of the functions relating to perception. One of the latest assumptions is that motor difficulties might be caused by a problem with controlling visuospatial attention and, in particular, disengaging attention.
In addition to slowness of both planning and performing movements, these children often have more difficulties than is usual, for example, in regulating the strength needed in a finger-grip. This can be observed in a child using excessive gripping force in handwriting more frequently than is usual compared to his/her peers. Furthermore, problems with rhythmic regulation and timing impede changing the speed of movements according to instructions, or create difficulties in keeping pace with a given rhythm (e.g., skipping rope). It has also been suggested that coordination disorders develop because affected children cannot control their movements as precisely as others by using “efferent copy” of the movement in the brain. Children affected in this way have difficulties particularly with motor functions that demand using internal representations of movements (e.g., remembering movements or drawings, identifying hidden fingers). These findings provide new opportunities, particularly for applying methods based on using mental images in the remediation of coordination disorders.
Motor development
Although the basic motor and movement skills, including handling of objects, are learned during the first years of life, significant changes occur in the child’s motor development throughout schoolage. Developing motor skills are the foundation for the expansion of the child’s boundaries in life and for his/her meeting the surrounding world’s demands for increasingly precise, fine motor performance. It has been estimated that 30-60 % of the school day consists of activities that require fine motor skills such as, for example, using a pencil for writing or drawing, using a computer keyboard or mouse, or tying one’s shoelaces.
In school-age, children’s muscular control improves and movements become more fluent as they are automatized. Movement form also improves and diversifies. Improving balance skills and developing movement coordination lay the foundation for increasingly skilful performance and lively physical games. It is precisely the repetition of motor functions in play that strengthens the nerve connections that are the basis for developing skills. As the brain’s frontal areas develop and the connections between the frontal and rear areas are strengthened, the planning and controlling of motor activity develops as well, improving the child’s ability to take changes in the environment into account and to regulate their movements according to the situation.
The foundation for voluntary movements is a complex and multilevel functional system in the brain. The starting point for activity is intention or a motor task, which creates a pre-action “actionresult model.” Depending on the situation, the same motor task can be performed with very different movements and thus with different nervous system processes. Because the human organs for motion offer nearly limitless possibilities for performing a certain movement, a successful movement requires real-time information regarding the changing limb positions and the state of the muscular system. This is why kinaesthetic and visual feedback information is especially significant for successful movements. In this functional system, which is the basis for voluntary movements, each different area and functional level of the brain has its own task necessary for movements.
Motor difficulties, the environment, and interaction
Motor difficulties manifest themselves in many ways in the child’s social, physical, and cognitive development. The limitations caused by abnormalities or slowness of motor development impede the child’s getting acquainted with the surrounding world and restrict their social interaction. Pronounced motor difficulties can affect the child’s nonverbal communication (producing and understanding gestures, expressions, and body language in general) or the child’s behavior and movements in such a way that it draws negative attention from the other children, who in turn can be a partial cause for the child being left out or bullied. Difficulties may also manifest themselves in the child’s reluctance towards lively games that demand physical activity, which are important for the child’s development, learning of social and motor skills, as well as for their fitness. Thus, the choices concerning everyday activities often strengthen the original problem because the child is left without the necessary practice in skills that are particularly difficult for him/her.
Encouraging and directing the child into environments, games, and fitness activities that support motor activity requires determination as well as a considerate manner of instruction from the adults. Many studies reveal how clumsiness is a risk factor increasing low self-respect and feelings of inferiority. Early detection of motor difficulties makes it possible to avoid such courses of development.
Assessment of motor functions
Assessing motor skills has significance for learning disability research in at least three ways. Firstly, it is significant for diagnosing and assessing motor development disorders as a basis for planning remediation. The goal is to determine whether the child’s motor difficulties are so obvious that they impede, for instance, the child’s daily life, school attendance or engagement in hobbies, as well as to assess to what types of specific motor skills or background factors the difficulties pertain. Its second significance, which is often emphasized in neuropediatric research, has to do with the role of motor and sensomotor functions as indicators of possible development disorders in the child’s nervous system. This kind of research often seeks various neurological signs (e.g., very distinct side effects or abnormalities in muscle tone or reflexes, or difficulties in diadochokinesis tasks that evaluate rotation of the hands) that reveal disorders or underdevelopment in the nervous system. Many of these so-called “soft neurological signs” are symptoms that can be considered abnormal in respect to the child’s age (e.g., associated movements of a younger child compared with those of children over ten years of age, or difficulties performing serial movements). The third significance, albeit related to the previous ones, is that motor skill research can be seen as part of a thorough neuropsychological assessment that describes a child’s strong and weak areas of development.
Quite simple methods can be used for the purpose of determining whether a child can be considered clumsy and a larger group of children can be screened for motorically more slowly developed children to be selected for closer assessment. Diary-type methods based on parents’ observations have proved useful in monitoring early motor development. In a Finnish follow-up (Ahonen, et.al, 2004; Cantell, et.al., 2003) study of five- to eleven-year-old children, the small-scale motor analysis included in the examination of five-year-olds at child health clinics has also been noted to screen motorically challenged children quite reliably. Even though the official ICD classification recognized in Finland requires the use of a standardized test for the diagnosis of a motor skill development disorder, in practice this happens relatively seldom. Normally the diagnosis is based on observations of the child’s motor skills, gathered from various sources. In psychological examinations, the assessment of fine motor and visuomotor skills is often emphasized. Neurological examinations and tests performed by physiotherapists or occupational therapists often provide a more precise picture of children’s motor skills, balance and positioning skills.
Planning and performing movements requires sensing the positions and movements of various body parts, as well as precise observations of the environment around the activity. This is why the connection of visual and kinaesthetic perceptions and executive functions with motor difficulties should also be considered when making an assessment of motor skills. According to many clinicians, assessors of motor skills should try to determine whether motor coordination problems are more centred on planning activity (i.e., the child does not really know how something should be done or in which order the movements are to be performed – dyspractic difficulties) or performance activity (i.e., the child knows what should be done, but performance is arduous and/or inaccurate – motor difficulties or clumsiness). Making a clear distinction is not always possible, and often these difficulties appear together.
An example of the systems of examination in use is Henderson and Sugden’s (1992) “Movement ABC” (Movement Assessment Battery for Children). It has been designed particularly for four- to twelve-year old children, and it evaluates motor skill subcategories like finger dexterity, static and dynamic balance, and ball skills. At present, it looks like Movement ABC has become the central method for the diagnostic assessment of coordination disorders. There is also a small volume of Finnish reference data for the test. Even though the Movement ABC is relatively brief (20-40 minutes), its high cost is probably what has hindered it from being even more widely adopted.
In studying fine motor skills and finger dexterity, Tiffin’s (1968) Purdue Pegboard Test has proved useful, and good normative data concerning children is available for it. In the test, the child must place metal sticks into holes on a board separately with both hands, and then with both hands at once. In addition, the test includes an assembly task that measures hand coordination, rhythm, and alternation. Neuropsychologically, the test offers precise reference data on the comparative functioning of the body’s left and right sides.
Although the NEPSY and NEPSY II test battery, which is well-established in children’s neuropsychological testing, contains a geometrical design-copying task, many psychologists still use Beery’s (1997) VMI test to assess visuomotor performance. The merits of the test are the precise developmental order of the designs and the additional tests of visual perception and motor coordination. Rey’s Complex Figure test (CF) tasks of complex figure copying and reproduction from memory are more complicated, but in many ways interesting. In Rey’s test, observations are made of the child’s strategy and its effectiveness (getting stuck on details, or using fragmented- vs. whole-perception) by changing the color of the pencil the child uses for copying at certain intervals (Waber & Holmes, 1985).
Regarding these tests, it has been suggested that it would be possible to evaluate the status of the executive functions necessary for visuomotor performance by comparing the child‘s performance on the Rey and VMI tests. If the child performs clearly better on the VMI test than on Rey’s more complex test, then problems with executive functions could be assumed, at least in visuomotor performance.
NEPSY subtests that measure motor skills, visuomotor skills and the sensory system, are namely: Oromotor Sequences, Fingertip Tapping, Imitating Hand Positions, Visuomotor Precision, Manual Motor Sequences, Finger Discrimination, and Design-Copying. Visuospatial (Arrows, Block Construction) and planning (Route Finding) tests can also reveal additional information on the factors behind motor difficulties. Earlier versions of NEPSY contained subtests (e.g., a task that measures motor control with speech, and finding arm positions without visual feedback) that have proven extremely useful in assessing motor skills, but are no longer included in the newest version.
Motor development disorders are quite permanent and they are also related to other problems in the child‘s development. This is why it is so important to make as early and reliable a diagnosis as possible, as a starting point for supporting the child’s motor development. To date, there are several reports on motor coordination disorder remediation (Wilson, 2005), which offer clues as to how motor difficulties can be observed in different daily situations and what kind of approaches are available for remediation.
TABLE 24
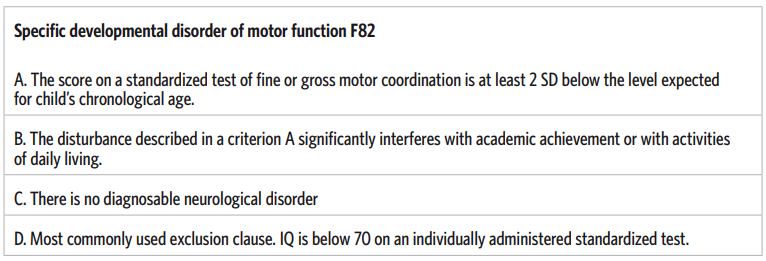
References
Ahonen, T., Kooistra, L., Viholainen, H., & Cantell, M. (2004). Developmental motor learning
disability. A neuropsychological approach. In D. Dewey & D.E. Tupper (Eds.) Developmental
motor disorders. A neuropsychological perspective (pp. 265– 290). New York: Guilford.
Beery, K. E. (1997). Beery-Buktenica Developmental Test of Visual Perception and Motor Cordination
(4th edition, revised). Administration, scoring and teaching manual. Parsippany, NJ: Modern
Curriculum Press.
Cantell, M., Smyth, M., & Ahonen, T. (2003). Two distinct pathways for Developmental Coordination Disorder: Persistence and resolution. Human Movement Science 22, 413–431.
Henderson, S.E. & Sugden, D.A. (1992). Movement Assessment Battery for Children. Kent,
UK:Psychological Corporation.
Tiffin, J. (1968). The Purdue Pegboard. Chicago, IL: Research Associates, Inc.
Visser, J. (2003). Developmental coordination disorder: a review of research on subtypes and comorbidities. Human Movement Science, 22, 4-5-, 479-493.
Waber, D. P. & Holmes, J. M. (1985). Assessing children’s copy productions of the Rey-Osterrieth
Complex Figures. Journal of Clinical and Experimental Neuropsychology, 7, 264–280.
Wilson, P.H. (2005). Practitioner review: approaches to assessment and treatment of children
with DCD: an evaluative review. Journal of Child Psychology and Psychiatry, 46, 8, 806–823.

Tuija Aro, Sydney Mwaba, Mwiya L. Imasiku and Ecloss Munsaka
9. Memory functions
How are memory difficulties manifested?
It is often said that children do not have memory problems like adults do. However, many professionals say that children with learning disabilities often have poor memory as well. Teachers may report, for example, that the child forgets instructions or objects, or that his/her learning is irregular. In other words, today the child cannot remember things that he/she mastered yesterday. At home the parents may observe similar forgetfulness. For instance, when asked to do two things, the child will forget one of them. Is such a case a problem with memory, attention, or both? And if it is a memory problem, what kind of memory performance is impaired?
Even though actual long-term memory developmental problems are not usually observed in children, there may still be significant differences in their ability to keep items in mind or recall things. These differences certainly have implications for children’s learning. Many studies have also associated difficulties observed in memory tests with difficulties in learning, such as dysphasia (SLI), dyslexia, and Attention Deficit Hyperactivity Disorder (ADHD); these have usually been cases of so-called working memory, which are described in this chapter in relation to learning disabilities.
What causes memory difficulties?
Memory can be defined in many ways. Regardless of the definition or theoretical model, the central factors can be seen to be the ability
- to make observations and to focus attention on the essential information,
- to analyze and process information,
- to memorise, or to store information, and
- to recall information.
The first stage has much to do with attention as well. The child must be able to select the matter to be memorised and processed, and focus and maintain his/her attention on it. In the second stage, the child processes the remembered matter. The concepts “deeply processed” or “superficially processed” are used at this stage. These refer to how it is easier to recall information later on if it has been deeply rather than superficially processed. In the storing stage, information is transferred to long-term memory, from where it is, in principle, always retrievable. In the recalling stage, a person seeks information from his/her memory. The retrieval process requires monitoring the correctness and accuracy of the information retrieved. The success of memory retrieval is closely connected with strategies and the ability to classify information.
According to many theories, information is first received in a sensory store. The information in the sensory store is thought to correspond quite precisely with the physical stimulus (picture, letter, or sound series), which stays in mind for a few seconds. According to research, learning disabilities do not seem to involve difficulties in this working stage when information is in the sensory store. However, some studies have associated difficulties in identifying rapidly presented information with ADHD (Alloway & Gathercole, 2006).
From the sensory store, the information is transferred to short-term memory, where it is stored slightly longer. Short-term memory is closely related to attention and it has only limited capacity. Short-term memory can be seen as an instrument of human information processing; with it, we maintain information for short periods. Traditionally, short-term memory is assessed with tasks in which the child must remember numbers, words or shapes in either a free or given order.
In particular, problems remembering serial verbal information have been associated with learning disabilities. Weaknesses in retrieving familiar units, such as letters, words and numbers, have been associated with dyslexia in particular. This may be explained, for example, by an observation made in some studies, that children with learning disabilities make deficient use of activating mental images of words. In other words, their use of memory is less strategic than that of their peers.
In colloquial language, working memory is often used as a synonym for short-term memory. However, according to theoretical models, short-term memory and working memory are (at least partially) separate functions. The theories suggest that working memory tasks require simultaneous performance of cognitive functions, unlike short-term memory tasks. Thus, the aforementioned tasks that require mere repetition are not actually working memory tasks. According to memory researchers, only speculative deductions can be made regarding a person’s working memory (the central executive and phonological loop, described next), on the basis of number series repetition.
The working memory model of Baddeley and Hitch (1974; see also Gathercole & Alloway, 2006; Swanson & Sáez, 2003) is probably the most well-known. It suggests that working memory consists of the central executive and so-called slave-systems. The central executive cooperates with these subsidiary systems. Each of the subsidiary slave-systems processes different material. The system known as the phonological loop processes phonological information, and the system known as the visuospatial sketch pad processes visual and spatial information, divided into the static (location) and dynamic (movement) sections. In addition, the model includes the so-called episodic buffer, which is responsible for combining the information from the subsidiary systems and longterm memory.
Traditional short-term memory tasks require the use of only one subsidiary system and do not assess the capacity of working memory as a whole. The functioning of the phonological loop is usually assessed with non-word or number series memory tasks, and the sketch pad with tasks that require memory of spatial location or unfamiliar visual figures. There is still controversy among researchers about the assessment of the episodic buffer. Working memory difficulties present themselves in the daily work of children and adolescents as, for instance, difficulties processing material in the mind and concentrating on several things simultaneously. This often makes children sensitive to distractions as they work. Working memory problems are typical in connection with Down syndrome (especially the phonological loop), Williams syndrome (spatial memory), and language development difficulties (phonological loop and central executive).
The capacity of long-term memory is boundless and it stores information based on meanings. The material that is transferred to long-term memory is largely determined by control processes. Information storage in long-term memory is affected by the used mental associations, relations, and organising plan. Research has associated learning disabilities with ineffective memorising strategies and deficient recalling processes. Poor study strategies and self-knowledge as a student, as well as difficulties processing subject matter, make it strenuous for children with learning disabilities to commit things to memory. Or, for its part, if the memorised matter is poorly organised, it is arduous to recall.
To summarise, it can be said that children’s memory difficulties often have to do with insufficient working memory capacity, which is hard to distinguish from difficulties with attention capacity or effort. This is seen in the difficulties described before, keeping in mind several things simultaneously and the tendency to concentrate on one individual characteristic of available information. Difficulties processing information in working memory hinder organising information and transferring it to long-term memory. In addition, children’s difficulties in organising information and making use of effective memorising strategies cause information to be stored in longterm memory in a poorly organised manner, making it difficult to recall.
Low performance in memory tasks may also be caused by other factors. Central factors to assess are, for example, the child’s or adolescent’s language functions (including e.g., vocabulary, hearing), executive functions, and their general performance level.
Development of memory functions
Memory functions develop with age, mainly through the developing control processes, inhibition and awareness. A person’s ability to select what is essential to commit to memory from among the flood of stimuli in the surrounding environment improves. Likewise, the child’s ability to consciously process and organise information in his/her mind develops, facilitating storing to and retrieving from memory. Because working memory is closely connected with attention and the development of the frontal parts of the brain, which still continues during an individual’s second decade in life, it is understandable that working memory also strengthens at this time. Some theories suggest that the improvement of working memory also concerns the mental ability to repeat and to practise the units to be memorised, in which case the length and repetition speed of the units are significant. Children acquire this skill at around seven years of age. However, there seems to be quite a lot of normal variation in each of the elements of working memory during every age level. This is plausible, considering how many factors affect memory development.
Age, therefore, brings both qualitative and quantitative development. Some functions are automatised, the ability to filter out inessential things develops and thus the child’s sensitivity to distractions is reduced, and his or her ability to use strategies improves. The child’s memory development is seen in the use of strategies and their effectiveness. Strategies develop along with age and, for example, language development. This can be observed in the child’s ability to use different memory supports based on classification and organisation. It is also significant how well the child or adolescent understands what each task requires of their memory, and how they learn and remember things best (so called metamemory).
The significance of memory for learning
In the child’s daily life, the quality of his/her memory is verified by the ability to commit things to memory and to recall the right things at the right moment. In school learning, different memory functions are constantly in active use (see also Gathercole & Alloway, 2006). Short-term memory is needed, for instance, for comprehending what is being taught and following instructions. Problem solving and information processing are both dependent on working memory. Material and events are consciously and subconsciously stored in long-term memory and retrieved when necessary.
Basic arithmetic information and knowledge of mathematical rules are also stored in long-term memory. Thus tasks that demand remembering multiplication tables or quick recalling of an addition’s sum or other calculation rule require retrieval from long-term memory. Working memory, for its part, is especially significant in solving mathematical problems, as the child must keep in mind many things and perhaps recall solutions to subcalculations from long-term memory simultaneously.
In colloquial discussion, working memory is associated particularly with mathematical performance. This connection may be related to the fact that limited working memory capacity restricts solving mathematical problems or inhibits the ability to learn, or in other words, to transfer the necessary facts and rules to long-term memory. It is also possible that limitations of working memory impede information retrieval from long-term memory. According to Baddeley, of the working memory components, the episodic buffer is necessary for the development of arithmetic skills, mental calculations and tasks that require mastering the number sequence. It has been suggested that the phonological loop also participates at least in the development of arithmetic skills. In addition, difficult mental multiplications employ the central executive, but not so much the visuo-spatial component. According to studies of visuo-spatial working memory, especially the static part of the sketch pad is linked with mathematical performance at school.
Working memory is also vital for learning to read. The phonological loop is especially significant for the development of word recognition and decoding skills, but the nature of this connection and the reason for its significance are not fully known. Because phonological memory is strongly connected with phonological awareness, it is difficult to develop a task that assesses phonological memory exclusively. On the other hand, solving strategies for phonological tasks change, and solving skills improve as literacy develops, which further hinders understanding the nature of the relation. Rapid naming is also linked with word recognition and decoding skills, and it is probably related to the effectiveness of both phonological working memory and phonological long-term memory.
Phonological working memory is also significant for learning vocabulary in one’s mother tongue or foreign languages. The more flexible the child’s phonological working memory, the better his or her ability to process new phonological combinations and to commit them to long-term memory. And the more automatised the phonological working memory, the more resources the working memory has, as it were, to concentrate on the meanings of language, and the better the understanding of language. The central executive, for its part, has to do with activating vocabulary and keeping a sentence in mind, and thus more with understanding the content of a sentence than with remembering its phonological structure.
In studies of working memory and short-term memory, problems with working memory have particularly been associated with reading comprehension difficulties. Apparently the importance of working memory for understanding text being read has to do with the vital role of the central executive in keeping material in mind, processing language and finding meanings. It is believed that people process so-called elementary thoughts on texts in their working memory and combine them into higher-level thoughts, which in turn are concentrated into a few main issues and themes. Although research has closely associated working memory with reading comprehension, other factors such as language functions and reading and memorising strategies are more significant for reading comprehension. These are especially significant for remediation and teaching because proper strategies support the weak working memory. The assessment of memory is described in the following table.
The table describes some of the central concepts often used in memory theories and connects them with broadly used tests.
Table 25. Assessment of memory functions
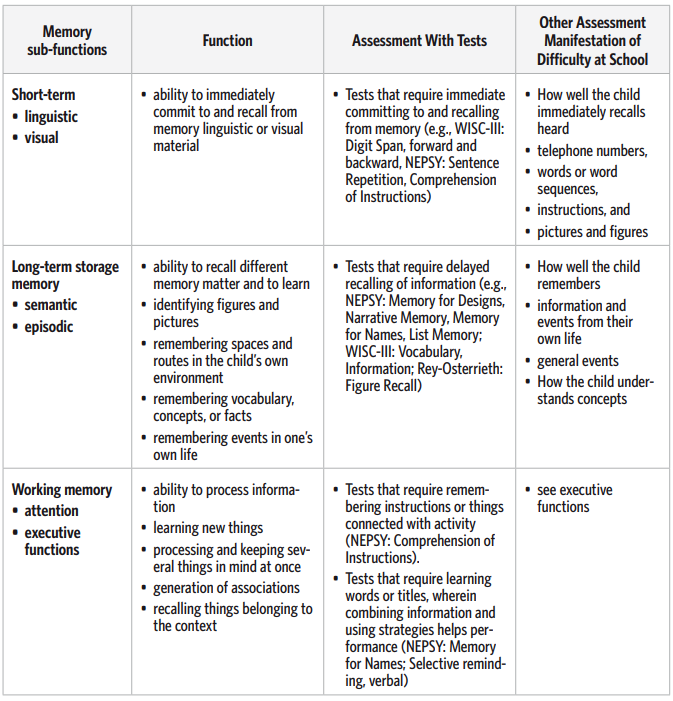
References
Alloway, T. & Gathercole, S. (Eds.) (2006). Working Memory and Neurodevelopmental Disorders.
Hove: Psychology Press.
Baddley, A.D. (2001). Is working memory still working? American Psychologist, 56, 11, 851–864.
Baddeley, A.D. & Hitch, G. J. (1974). Working memory. In G. Bower (Eds.), The Psychology of
Learning and Motivation, vol 8, (pp. 47–90). New York: Academic Press.
Baddeley, A.D., Gathercole, S., & Papagano, C. (1998). The phonological loop as a language
device. Psychological Review, 1, 158–173.
Buschke, H. & Fuld, P.A. (1974). Evaluating storage, retention, and retrieval in disordered memory and learning. Neurology, 11, 1019–1025.
Gathercole, S.E. & Alloway, T.P. (2006). Practioner’s review: short-term and working memory impairments in neurodevelopmental disorders: diagnosis and remedial support. Journal of Child
Psychology and Psychiatry, 47, 4–15.
Pickering, S.J. (Eds.) (2006). Working Memory and Education. A volume in the educational psychology series. London: Academic Press.
Schneider, W. & Björklund, D. (2003). Memory and knowledge development. In J. Valsiner & K.J.
Connolly. (Eds.) Handbook of Developmental Psychology. London: SAGE Publications Ltd.
Swanson, H.L. & Sáez, L. (2003). Memory difficulties in children and adults with learning disabilities. In H.L.
Swanson, K.R. Harris, & S. Graham, S. (Eds.), Handbook of Learning Disabilities
(pp. 182–198). New York: The Guilford Press.
Waber, D.P. & Holmes, J. M. (1985). Assessing children’s copy productions of the Rey-Osterrieth
Complex Figures. Journal of Clinical and Experimental Neuropsychology, 7, 264–280.
Mika Paananen, Pamela February, Cynthy Haihambo, Job Hengari,
Andrew Möwes, Daniel Muindi, Jacinta Kwena and
Carol Suzanne Adhiambo Otieno
10. Making conclusions and planning support
Aspects to consider when selecting essential information from assessment data
During learning disability assessment, a volume of information is gathered about the child. This information is used by the psychologist, teachers and parents to plan how to support the child in the future or to determine what possible further assessments should be made. Because of the vast amount of data, some of the data may seem contradictory. The most challenging task of the professionals is probably to identify the central and reliable data and to understand what best describes the child’s situation. The goal of assessment is usually to understand the phenotype problem and to obtain information about the causes of the problems. Sometimes the assessment disproves non-professional assumptions by replacing them with new information and new explanations, or it may confirm and help to classify the thoughts of those who know the child well. In some instances parents might tell you that their child finds it difficult to study, or the learners themselves can tell you with which tasks they have difficulties, such as remembering things. There have also been some instances where parents have indicated that their child is too lazy to study. Comments like this are normally made by parents who do not have specialised knowledge and in extreme cases may not have had the opportunity to attend formal education.
In the beginning of this book, we presented a model for gathering and organising information, which proceeds on four different levels. Firstly, learning disability assessment begins with descriptions of the child’s activity and behaviour, or in other words the phenotype, which generates the first assumptions to be tested. Secondly, knowledge of the child’s developmental history offers more specific information about the history and possible causes of the difficulty. Developmental history is often an important source of information in questions of differential diagnosis. Thirdly, the assessment of cognitive functions and academic skills offers detailed information on the nature and causes of the difficulty. Tests, observations, and informal assessment methods and materials are the most central tools of assessment on this level. Fourthly, assessing environmental and interactional factors gives the assessors a more general picture of the child’s life situation. They define how the problems manifest themselves in the child’s life, as well as guiding the appropriate support to plan for each child. This four-level model is helpful in learning disability assessment because different developmental problems and learning disabilities present themselves in different ways on the different levels of assessment.
The previous chapters have described the development of functions and skills, abnormalities, and characteristics of phenotypical problems. The next section will examine decision-making based on test results, observations, environmental, emotional and interactional factors.
Test results must be associated with phenotypic difficulties
A central principle of interpretation is that assessment must be based on several corresponding observations. A child’s poor performance in an individual test or situation may be coincidental and not necessarily an indicator of a disability. Verification of a disability therefore requires other parallel or additional observations during the same assessment or from earlier assessments to be considered. Confirmation can be acquired by having the child do other tasks that assess the same cognitive function, or by observing situations where the problem is likely to surface. The child’s developmental information may also be used to confirm or disprove such assumptions. Other people who work with the child may be asked if they have noticed similar occurrences.
The assessment’s observation data should reflect the child’s activity in his or her own environment. By combining observations from different sources with the test data, conclusions can be made regarding which cognitive functions might explain the observed difficulties. This also creates an opportunity to determine to what extent the problems may result from cognitive difficulties and what part environmental and interactional factors may play. Combining observations and test data provides more reliable information for the planning of remedial support and finding essential procedures.
The child or adolescent may have been referred for learning disability assessment because of only one problem evident on the surface level, but in the cognitive profile based on the assessment, deficits are then observed in several functions. This can be seen in connection with syndrome-type difficulties such as Nonverbal Learning Disability (NLD), but sometimes also with individual learning disabilities. In such cases, the assessor seeks neuropsychological connections between difficulties observed in different functions. This helps the assessor to understand the nature and causes of the learning disability. For instance, in learning to read, a child may have difficulties with cognitive functions such as naming, language fluency, linguistic working memory and even oral motor skills. All of these are probably related to a child’s difficulties in learning to read. Alternatively, if the child is confirmed to have extensive deficits, for example, in vocabulary, morphology or inflections, if the language includes inflectional morphology (like in Finnish, Kiswahili, Afrikaans or Otjiherero) or syntax, then it is probably a broader language difficulty than dyslexia.
Sometimes a child or adolescent is referred for assessment because of several difficulties apparent in his or her phenotype. In such cases, the child probably has deficits in several cognitive functions. For example, simultaneous reading difficulties and fine motor skill problems observed in daily life may be seen in tests as difficulty with rapid naming or as slowness and inaccuracy in tasks that require fine motor skills. Attention-Deficit Hyperactivity Disorder (ADHD) often presents itself simultaneously with other developmental problems and learning disabilities like dyslexia. According to some studies, these difficulties are independent and hence not in direct cause-effect relationships with each other. This thinking emphasises the fact that the core difficulties (phonological problems and difficulties with executive functions) of both problems (e.g., dyslexia and ADHD) in the child’s cognitive performance are seen to be like those of children with only one of the difficulties in question. Following this thinking, scientific research has shown that neither difficulty has caused the other – dyslexia is not caused by attention problems, or vice versa.
On the other hand, due to the fairly unspecific nature of developmental disorders and the amount of overlap, the possibility of a common background cause has also been increasingly investigated. This alternative is represented by, for example, the concept of Atypical Brain Development (ABD). ABD comprises a broad variety of developmental and academic problems that are often observed to coincide in children and adolescents. An assumption in the ABD approach is that abnormal organisation of the child’s neural network (probably due to genetic factors) also generates abnormal brain activity, which then appears as various behaviour and learning difficulties. Therefore, it seems that some children have only one, some two, and some several difficulties that need to be systematically assessed.
Neuropsychological theories guide the interpretation of assessment findings
The child’s performance in cognitive tasks can be approached from different perspectives. Normally, in the first stage of assessment, the child’s development and abilities are examined as a whole. Comparing the child’s performance with normative data of their peers reveals if it deviates from the typical performance of the age group. In many African countries, there is a need to identify age-appropriate norms across various cultures. Currently, the assessment norms being used either originate from South Africa or the West. Sometimes it is noted that the child’s development and abilities are weaker as a whole than their age group, and that the child has extensive deficits in their learning ability. Substantial regression in a reliable test – which is actually quite uncommon – may be a sign of a progressing nervous system disease. In such a case, a child neurologist or paediatrician must perform an examination. If it is a question of a learning disability in the traditional sense, then there may be no significant deficit in the child’s overall skills (e.g., general IQ), but instead the difficulties appear in relatively limited areas of cognitive functions (e.g., rapid naming or verbal working memory).
Specific difficulties can be found by examining the child’s performance profile and comparing the performances in the different functional areas (language, attention, memory, visual, spatial and motor functions). This reveals how the different areas have developed and how they function in relation with each other. The assessor can see if there are significant differences that may be signs of particular abnormalities in the learning or development of a specific function. These observations are interpreted in relation to each other and to the difficulties observed in the child’s activity and behaviour (i.e., the surface level). At the same time, the strengths in the child’s skills can be distinguished, and it is warranted to highlight them and make use of them in teaching. Particularly in seeking a neuropsychological connection between observations, one must keep in mind that the successful performances and “strengths” are also significant. They are interpreted in relation to the poor performances. This either confirms or disproves assumptions about the failure of a specific function.
In learning disability assessment, the neuropsychological approach offers one possible interpretation in the form of brain activity and development data. Nowadays we know quite a lot about brain functions and the specific consequences of various types of brain damage in developed (adult) brains. However, the consequences of damage to developing brains are often different and harder to predict. The greater challenge for research is to try to understand how brains that have developed abnormally from prenatal times make use of the environment’s stimuli, how they process learning, and how the learning results can be recognised using certain assessment methods. Developmental neuropsychological research attempts to shed light on this challenging area, for instance combining neuropsychology and developmental psychology, bearing in mind that the brain always develops and functions in a specific context.
One of the central neuropsychological approaches to testing results and observations has traditionally been to examine differences between the two hemispheres of the brain. There is reason to always perform this examination in the assessment of children and adolescents. In the context of tactual and motor tasks, the assessor should compare the performance of the right and left (dominant and non dominant) hemispheres. This provides data on the possible differences between brain hemisphere functions. Right- or left-handedness, at least for simple motor tasks, is presumably established by 5–8 years of age. The left-right differences can also be observed in visual perception. For example, in tasks involving visual searching, the child or adolescent may favour one side, begin drawing unconventionally from the other side, or build the other side last. Signs of damage to the left hemisphere may hence be seen in the form of, among other clues, weaker language functions than visual functions, weaker motor and tactual performance of the right hand than the left, deficits in the right visual field, and sensory deficiencies in the right hand when touching both hands at once.
While interpreting observations, it is also good to keep the brain’s functional units of Luria’s model in mind (Luria, 1973; see further on). These units help us understand the functional differences between the deep and surface areas of the brain, the significance of the connections between them, and the role of the front and rear parts of the brain. Luria’s model of brain functions is also the foundation of the NEPSY II test battery. Today, it is known that the brain’s information processing is not quite as hierarchical as Luria’s original model assumed, but rather, the cortical areas have reciprocal connections with each other – and with the subcortical areas as well. Hence, the cortical areas are also presumably involved with several functions and actively affect each other. As experience accumulates, the connections form neural networks that consist of both internal connections within the cortical area and connections between different cortical areas.
Box 5. Neuropsychological approach to the assessment and interpretation of test results
The first functional unit of Luria’s model comprises mainly the reticular formation, or for instance, the brainstem and the thalamus, which have bidirectional connections with the cerebral cortex. The main task of this unit is to maintain alertness and activation levels, but it also participates in the regulation of reflexes, muscle tone, breath, and the heart. It screens the signals from the outer world, the body, and for example the frontal lobe, as well as adjusting the rest of the cerebral cortex based on those signals. Thus it makes it possible to sustain the correct alertness and activation level, as well as selective attention. The concept of an ascending activation system is used for the signals from the outer world and the body. The signals returning from the cerebral cortex to the reticular formation are referred to as the descending activation system. Damage to this unit causes problems with alertness and attention, among other effects. It may also cause problems with learning and memory.
The second functional unit is formed by the hind parts of the brain, or the parietal, occipital, and temporal lobes – including the cerebral cortex of these areas, and the manifold connections with the structures under the cerebral cortex and other brain areas. The task of this unit is to receive, interpret and store information. Damage to the areas of this unit may be quite diverse according to the location of the functional problem. The third functional unit is the frontal lobe, which plans and implements functions in relation to the observations and intentions of the individual.
Luria also divided the brain areas in the second and third functional units into different functional levels (primary, secondary and tertiary). The so-called reception or primary areas in the second functional unit receive signals from sense organs. The reception areas contain quite specialised cells that react only to certain characteristics of stimuli. From here the stimuli are transmitted to the combining areas, also known as secondary association areas, where they are further processed and combined into an overall impression and meanings begin to be attached to the stimuli. According to Luria’s model, the higher association areas, i.e. the tertiary cortical zones, combine the data processed by the different brain regions. This is the most challenging function, which requires many different kinds of connections.
The reception areas of different sense organs are located in different cerebral lobes. Sight is in the inner and rear regions of the occipital lobe, hearing is in the temporal lobe, and touch and feel is in the parietal lobe behind the central fissure. Damage to these regions causes partial or complete sensory deficits. The sensory association areas are located in the immediate vicinity of the reception areas. Damage to these areas causes perception difficulties, or difficulties perceiving sensed data (forms of agnosia). The higher association areas, for their part, are situated in the barrier layers of the cerebral lobes, in their joint zones. Because they are the youngest areas in species’ and individual development and are responsible for the most demanding functions, damage therein affects neuropsychologically non-specific functions such as language comprehension and mathematics.
In the frontal region of the brain – Luria’s third functional unit – there is also the primary motor cortex, which is located right in front of the central fissure. It corresponds to the reception area of the second functional unit in the hind parts of the brain. Functionally, this region is responsible for transmitting movement signals to the muscles of the opposite side of the body. Damage to this region may lead to paralysis or paresis. In front of the motor cerebral cortex sits the premotor cortex, which corresponds to the association areas of the second functional unit. It controls smoothness of movement, and damage to this area causes faltering and staccato movements – movement is not smooth or flexible (e.g., NEPSY: Manual Motor Sequences, Oromotor Sequences). Damage to the premotor area also impedes the regulation of voluntary movements. Broca’s area, historically well-known in the field of psychology, is also a part of the premotor area. It is especially significant for fluent speech production.
In the very front of the brain is the prefrontal area, the higher association area of the third unit. Its central tasks are executive functions, setting goals, and planning, based on the combining of data from elsewhere in the brain, body and environment. The prefrontal area’s extensive connections, such as through the reticular formation to the second functional unit, make two-way information flow possible. Damage to this area leads to difficulties with executive functions, conflict between actions and intentions, and difficulties in evaluating and correcting one’s own activity. If there is damage to the lower parts of the frontal lobe, or the so-called basal areas, the person has difficulties, for example, in controlling their fits of temper, and sometimes even their motor impulsiveness.
One neuropsychological approach based on Luria’s theory is to examine whether functions require activity of particularly the front or rear regions of the brain. Functions of the rear regions are those of the second functional unit, and those of the frontal region are primarily the third functional unit’s functions, or tasks that demand planning and implementing activity (such as motor skills, speech, and executive functions). For example, it is known that linguistic neuropsychological symptoms are caused by damage to the second functional unit area (e.g., comprehension difficulties) and to the deeper regions. But the third functional unit is also essential for functions pertaining to language production, such as formulating thoughts and objectives into words, or smoothness speech movements.
An approach that has often been proven fruitful in learning disability assessment is the analysis of the internal structure of a function (subcomponents of the functional system in Luria’s terms). For example, if a child has visuoperceptual problems, then there is reason to more closely examine the subcomponents of the function in question (e.g., visual attention, identifying an object or figure, detail observation, visuoconstruction, spatial perception). In this way, the assessor can form a picture of what kind of tasks are difficult for the child, which sub-processes their difficulty lies in, and which areas should be strengthened and made more use of in daily activities. This requires neuropsychological and cognitive theoretical knowledge of each function, which is only partially presented in this book, primarily in the tables.
Assessors must be critical
Specifically determining the nature of the child’s cognitive strengths and weaknesses and their connection to learning disabilities usually requires psychological, pedagogical and special educational assessment. In the tradition of psychological learning disability assessment, neuropsychological methods have been central. In the past, the goal of testing was to make assumptions regarding a brain activity disorder in one of the brain areas pointed to by the tests. Tests were done to reveal the existence of a disorder and which functions were impeded as a result. Nowadays, tests are used rather to obtain information on the strengths and weaknesses of the child’s performance level in different cognitive functions and to describe the efficacy of these cognitive functions in relation to the demands of tasks and school learning. The assessment clarifies the child’s difficulties in daily life and learning, and thus helps in understanding the underlying causes of the difficulties. However, for a reliable picture the assessment methods should evaluate cognitive functions extensively. On the other hand, there is an increasing attempt to apply knowledge of brain activity to observations and neuropsychological know-how to conclusions in order to make the observations more understandable.
Generally, standardised tests are used in cognitive function assessment and create a framework for psychological or pedagogical assessment. When tests are used appropriately and according to their purpose, they offer a good picture of the child’s development and skills. However, everyone should now and then critically examine the effectiveness of their own test methods and remember their limitations. Psychological cognitive function assessment methods, in particular, are believed to assess specific sub processes precisely. However, the tests always require simultaneous activity in several skill areas or sub areas. To find out what affects performance and how it can affect learning, the assessor must know which cognitive functions are engaged by the task.
A test may therefore be limited as an indicator of a specific cognitive function because most tasks demand simultaneous use of several different functions. This especially applies to WISC-III subtasks for instance, but also to several sections of the NEPSY. The NEPSY subtests have been divided into six functional domains: Attention and executive functions, language, sensorimotor and visuospatial functions, as well as memory and learning. In NEPSY II, the domains are: Attention and executive functions, language, memory and learning, sensorimotor and visuospatial functions, and social perception. For each of these domains there are tasks which help examine the functions as precisely as possible. All performances, however, are dependent on several subprocesses which do not belong exclusively to only one of these functional domains.
For example, it is hard to define specific test tasks with which Attention-Deficit Hyperactivity Disorder could be diagnosed. The various sub-processes of attention are necessary in all tasks, and during assessment the child’s attention faces many challenges. It is thus important to find a way to distinguish the task’s demands on cognitive functions and to differentiate between these and the other challenges of the situation. It is essential to understand how various factors are related with the phenotypical problem. In addition to test data, this requires observations in assessment situations, developmental data, and assumptions regarding the primary difficulty, all based on interviews and the phenotypes. During assessment, the assessor must pay close attention to the child’s reactions, such as hastiness, discouragement, fatigue, fluctuating emotions, or excessive use of coping mechanisms. The assessor must also evaluate how these affect task performance. Situational factors and the quality of cooperation also affect performance.
The following question arises in testing: Is there a certain threshold value below which it can reliably be said that the child has a specific deficit in his or her skills or activity? Normative data should be available for most tests, which help determine the child’s performance in relation to his or her peers and provide information on possible skill deficits. But we know that there is still much to do in regard to collecting comparative and normative data in the African context. Usually, a performance that is more than one standard deviation (15.9% of the population on the weaker side) is enough grounds to suspect a skill deficit. However, the diagnostic criteria normally require that two standard deviations below the average have been observed in a performance or test before a deficiency in skills is confirmed.
Tests form only one part of assessments. The assessor must also compare test data with observations of the child in the child’s own environment in order to see which test results confirm themselves there. Assessment should be a comprehensive process that evaluates the child’s learning disabilities and life situation extensively with several methods and in cooperation between the psychologist, family and teachers. The assessors must not get stuck in a difficulty-oriented viewpoint, but must rather take note of the child’s strengths and their means of coping. Strengths can be made use of in planning teaching and remediation, and ways of coping and overcoming the basic problem can be built around these.
What may affect assessment results?
Emotions aroused in various situations, as well as earlier experiences of similar situations, always affect human activity. This also happens in learning disability assessments, even though the goal is for the child to succeed as far as is possible according to his or her skills. Learning problems may be combinations of deficits in cognitive functions, emotional factors that restrict the child’s learning, and weak learning strategies. The child’s executive function skills, his/her strategies, and the attributions he or she assigns to the situation are also significant factors affecting the child’s performance in tasks and assessment situations.
Furthermore, assessment must consider the child’s cooperation and his/her amount of effort, and the effect of these factors on the results. If the child’s effort is poor, the task results cannot be considered reliable data regarding the child’s actual skills. Observations of difficulties with exertion and lack of effort are important. A difficulty in some specific function (e.g., reading difficulty) often produces secondary problems (e.g., low self-esteem or lack of school motivation) that will have a negative effect on learning. Experiences and anticipation of failure may hinder exertion and effort. The child may already have developed a manner of avoiding tasks and may feel that the tasks are meaningless. This speaks for the child’s need for support in order to be able to trust his or her own skills, believe in his/her ability to learn, and to build up the courage to make an effort.
After the standard testing or assessment procedure described in the test manual has been followed, the assessor can deviate from the instructions and support the child’s performance with clues, questions, and instructions (cf., dynamic testing). For instance, the child can be taught an effective performance strategy for his or her particular situation. Then, the assessor can evaluate how the child or adolescent makes use of the given strategy, asking the child to describe how he or she solved the task and then making a note of how the child reasons. The assessor can also observe if the child notices his or her own mistakes whilst speaking. In this situation, the child or adolescent’s performance and test score is, naturally, not rated according to the instructions in the test manual as this part of the examination does not follow the standardised criteria for assessment. But the results obtained in this additional alternative way can be compared with the standard results. This offers clues as to what kind of instructions and support the child would most benefit from.
Performance in the assessment situation and at school is often similar. It is also possible that the child performs better in the assessment than in the classroom. This may occur in the assessment of academic skills as well as in psychological tests. In such assessments, the tests provide data pertaining to specific functions and skills in relation to the child’s age level, which can then be compared to the child’s performance at school. This reveals whether or not the child’s learning at school is progressing according to his or her abilities and skills. If a significant difference is noted, then this calls for determining what other factors hinder the child’s learning. These may be, for example, emotional reasons, illnesses like depression, or causes relating to interactive relationships between the school and the home. At the same time, learning motivation and self-image related issues may also be behind low performance, among other factors (see Figure 1).
What intervening factors, then, are most significant in planning support for children with learning disabilities? The beginning of the book describes factors that may impede learning. The same factors may deepen and expand the problems connected with learning disabilities. Sometimes problems can acquire a cyclic nature. These cycles can be roughly classified according to their scope. An example of a broad, negative, cumulative cycle is a situation in which the child’s difficulties are amplified by the parents’ inadequate instructional approaches and lack of consistency. When parents are confronted with difficulties in the child’s learning and their instruction, it can diminish the parents’ self-confidence in rearing the child. This, in turn, often impairs the parents’ instruction further and may create a negative tone during interaction, thus adding to the child’s existing learning difficulties. A similar cycle can form at school, between the teacher and child. In the African culture, it is expected of children to listen when adults talk and there is usually not an opportunity to question the adult’s instruction. This type of adult child relationship can also attach a negative stigma to interaction.
Negative cycles are formed on a smaller-scale between the learning disability and patterns of activity in task situations in connection with motivation. The learning disability produces failure, which weakens the child’s motivation and his or her will to make an effort. This usually leads to further failure, again decreasing motivation and effort. The goal of support is to prevent such negative cycles or to break those already existing, and to create positive experiences that increase the child’s will to learn and the instructing adults’ self-confidence.
Poor learning in comparison with cognitive abilities is often seen, for example, in connection with attention difficulties. More specifically, poor learning may be due to an inability to maintain attention for long periods of time, which also leads to being unable to work independently, especially on lengthy or complex objectives. These difficulties might not appear as poor performance in individual tests. In such a case, support should perhaps primarily be focused on the child’s attention skills and working strategies. In this way, the use of already existing skills can be improved in learning situations. Deficits in executive functions and working skills without a specific learning disability (in reading, spelling, writing, or mathematics) may also impede learning, and this to the extent that the student’s general performance at school can fall considerably below his or her general skill level.
From assessment to individual educational plan (IEP)
The starting point of an assessment is the learning problem observed in the child, making itself apparent when the child is learning more slowly than is usual for him or her, or for his/her age group, or through other unusual signs. As described earlier, learning disabilities are found in several areas of cognitive functions. Although it is known that there is a certain amount of regularity in learning disabilities, each child’s situation is unique. The combinations of cognitive functions and skill development features pertaining to learning are unique for every child. Children are different in both temperament and personality, and they also live in different psychosocial environments. All of these factors affect the individuality of learning disability phenotypes.
The focal point of support varies according to the child’s individual situation and the available forms of support. The emphasis is different with each child. The psychologist or teacher makes an assessment of the child’s general situation based on the available information in relation to the possible forms of support. The basis for assessment and decisions can be information on quite different levels; it can even be said that decisions and assessments are always made on the basis of partial information. Some amount of uncertainty must be tolerated. The child should, however, always be assessed from the viewpoint of increasing support and the environment’s resources. The Preliminary support planning form (see Appendix 1.) can be used to assess these aspects. The captured data on the form helps find the central areas in the child’s functions or life-situation that require support and assists the preliminary planning of the most suitable types of support.
How much knowledge is sufficient? A psychological assessment may have far-reaching effects, and the professional must be aware of his or her responsibility and understand the working methods involved. The assessment must be sufficiently broad in scope in order to find answers to the original questions: “Why is the child not learning as well as expected?” and, “How can we support the child/family/teacher?” In the method presented in this book, the viewpoint is that sufficiently extensive assessment considers the problem phenotype, the child’s development, test data, the social environment, and interactional or interventional factors. The assessment easily adds to the psychologist’s knowledge of learning disabilities and their manifestations in tests. The knowledge must also be applied to the child’s ecological environment, and the observations made in the assessment must also have been observed to occur there. Because finding an ultimate, isolated cause is not possible due to the diversified psychological and social phenomena involved, while planning support it would be appropriate to ask a further question: “What affects learning?” Through this type of question, it is easier to proceed towards concrete actions.
Feedback as a part of intervention
The foundation of cooperation with the child and his or her family is naturally a working model that respects the child and his/her family. In the African context, where the extended family plays a particularly significant role in child care, it is not always the case that the biological parents are the primary caretakers. At the same time, the procedures of psychological and pedagogical assessment are often unfamiliar to both parents and caretakers; the situations in assessment and feedback discussions may be new and strange to them and parents may not be sure of their role. In feedback discussions, the psychologist’s task is to remind those involved why the assessment is being conducted and to report the findings in connection with what has been done so far. In Namibia, for example, there are no mandatory multidisciplinary teams that discuss cases. In most instances, teachers directly inform parents during school-parent meetings about the progress or behaviour of their child. This is done in an informal way. In other instances, parents are called in by the school principal to discuss the student’s performance or behaviour. In most cases, only a school counselor, but not a psychologist, is additionally present and there is no fee. Only parents who can afford a private psychologist have the privilege of a professional psychological assessment and feedback, which would normally be conducted at a private practice. In such cases, parents will in turn inform the school about the psychologist’s assessment and feedback regarding their child, especially if concessions need to be made and intervention needs to be carried out by the school.
The observations made in the assessment should be presented openly within the parameters of the multidisciplinary team, nurturing the child’s self-image and anticipating support. Thus, the discussion concentrates more on the skills and functions that the child masters and what the child should practise and achieve, than on what he or she lacks; and in parallel, also placing more focus on what the family and teachers can do to support the child than on what has perhaps been left undone.
During this process, the child is appreciated regardless of his or her difficulties. The parents or caretakers are valued as the most important adults in the child’s life and their opinions need to be respected. In feedback discussions, the concerns and questions of the child and parents must be valued. It is vital to highlight the positive sides of interaction with the child and to emphasise the parents’ efforts and the effective solutions they have chosen to overcome the difficulties thus far. Often mere participation in the assessment and feedback discussions serves as intervention. There, the child notices that his/her parents and other adults care for him or her and want to help. The parents receive support and information whilst being assured that they are not alone in dealing with the situation.
The jargon spoken by teachers and psychologists is usually foreign to parents. Jargon is intended for internal communication within occupational groups. In feedback sessions, the professionals should use language that is understood by all stakeholders, as far as possible. Questions asked of the parents, as well as the opportunity for the parents to ask questions, help clarify unclear issues. Full understanding of the assessment results may also be difficult for parents, teachers, and the child. To present the results in a manner that is understood by all, it is good to trim and combine information and to emphasise the central observations. It is important to link the obtained data to daily observations and the parents’ and teachers’ accounts. Listening to the parents’, teachers’, and the child’s accounts of situations in which the difficulties occur and combining these with the data from the assessment tests bring the assessor closer to daily life and creates a coherent picture of the nature of the difficulties.
In some cases, there is uncertainty about the reasons and starting points for the assessment, and hence there is no clear goal for the feedback discussion. It can also happen that the discussion of the results becomes a monologue by the professional(s). This may typically happen in the African context, where parents may underrate the importance of their contribution to the assessment of their child. In such a case, it might be useful to go back in time in the process and review the starting points and reasons for referral to assessment, and the original concerns. Who was worried about what? Were the concerns different for the different parties? In this way, the roles of the different parties in the process can be defined and everyone can be committed and engaged in clarifying the child’s situation. Reviewing the original concerns and reasons for beginning the assessment helps to apply the obtained data to the child’s life circle and to the experiences of all involved parties.
The discussions may reveal that the occurrence of problems in learning has caused anxiety in the child or the parents. The conceptions, thoughts, fears, and hopes of the parents and the child are different in nature from the information that the test methods reveal to the assessor. The child or parents may fear being branded as abnormal or stupid. The parents may feel like they are being accused of their child’s difficulties and may feel the need to defend themselves. They may also deny the problems, or may not see or want to see any need for change or support. Eliciting and discussing these conceptions is especially important for the correct understanding of the child’s difficulties. Sometimes processing the issues may demand several meetings in order to reach a common understanding of all stakeholders.
It is challenging to give the child attention in feedback discussions where the parents, teachers, and psychologist are present. The situation often causes nervousness or even feels oppressive to the child. In most cases in the African context, it is expected of learners to be quiet and listen while their parents are talking to the teachers. In some instances, they are not even allowed to be present during such discussions. It is more comfortable for the child to receive feedback one-on-one or in a discussion with only the parents. In general, it is good to organise separate feedback discussions for the family and the teachers. In the family’s own meeting, it is possible to discuss things in confidence and to talk about things that might be missed in a discussion organised at the school. The feedback given to the child should be truthful and practical, and it should concern what hinders and what facilitates their learning. The issue can be approached, for example, by discussing the skill or school subject being practised. The emphasis should be on things in which the child is successful and on a par with his or her peers. The child should be encouraged to do his or her best and should be instructed in how to use working methods and strategies that are natural for him or her, in order to promote learning.
The problem is often defined and given a name (reading difficulty, mathematical learning difficulty, attention-deficit disorder, moderate language disorder, etc.). Naming the problem may be relieving and might improve the situation, especially if the child’s problems have been vague. The parents may have felt guilty for the child’s problems, or the child may have been accused of a lack of effort. On the other hand, named difficulties might be seen merely as abnormalities, which makes naming the problems feel like branding and does not necessarily increase understanding of the child’s problems. Another view might be that the learning disabilities or developmental problems are features of the child’s personality or ability traits which cause everyday coping problems in an education-centred setting, or which might not even be noticed in some other settings.
What makes naming the problems important is that it directs support. The child’s learning never ends, not even after a learning disability diagnosis. Defining the problem during assessment should not remain as a mere verdict of the situation, but it should create actions and interventions at school and at home. The purpose of feedback is not to isolate or classify the child, but rather to clarify the features of the child’s learning and to create opportunities for improved learning. However, forms of support, such as special education or remediation, may be felt to emphasise the child’s difference or isolate the child from the community. It must be remembered that a child with a learning disability feels different no matter what, and part of the feedback they receive concerns the anomaly and difficulty of their learning as caused by the disability. Assessment and feedback, as well as the ensuing support, do not add to being different as such, although they may temporarily increase the feeling of abnormality and being different. At best, they create understanding of the learning problems, support learning, create preconditions for improved learning performance, and reduce the possibility of falling further behind in learning.
Feedback discussions proceed from pedagogical and psychological assessment data towards concrete actions, which are more easily grasped by all parties of the discussion than mere test data. Based on the data accumulated during the assessment process, the assessor can determine the amount and nature of the support the child needs. Practical agreements, for example, on procedures and the amount of special education or classroom support to be provided can also be made on the same basis. Realistic learning goals can be set and pursued together. It is crucial to maintain and, if necessary, to increase the child’s and the parents’ – and in some cases the teachers’ – own responsibility and activity to solve the problems in each situation. The continuity of the process is also important. Parents and teachers (and possibly the therapists as well) should repeatedly engage in discussions regarding the child’s learning in order to monitor how well the child is progressing, and at some point they may also feel the need to set new goals to be achieved. At its best, this promotes the will to change the situation and creates positive cycles in which each party has experiences of success, which in turn feed the motivation to continue the effort to support the child’s learning.
The objects and methods of support
The observations and interpretations made during assessment, naturally, direct the choice of the forms of support. Support planners must also take the available forms of support into consideration, as well as what has already been tried and the extent of predictable future resources available to the child, the family, and the school. In addition, the environment where the child lives must be considered. These planned actions should be seen to focus directly on the child, the family, and the child’s class and school (see Table 26). As objects of support, the people or groups involved are not seen as alternatives or exclusive of each other. Support should be implemented on all necessary levels. The purpose of Table 26 is to demonstrate what can be done for the child on each level.
Special education and remediation are typical forms of support directly focused on the child. Their goals are usually to practise cognitive functions, to develop skills or knowledge, or to learn strategies that promote effective learning, or all of these. In special education, the focus is on academic skills. Choosing effective work and study strategies in appropriate situations helps and advances learning. Neuropsychological intervention emphasises cognitive functions and working strategies. Cognitive strategies are widely taught in learning disability remediation, and this usually has good results regardless of the skill in question. This does not mean that it is not worth teaching skills per se – for example, the only way to learn to read is by reading. Direct skill teaching is especially useful in areas where the developmental process of the skill is sufficiently known. In the African context, in the absence of sufficient professional support, it is important to identify what support is available within the school and at home. Peer support has proven effective in many ways. Peers are able to explain things at the level of the child, using methods or strategies that can easily be understood. At the same time, in the presence of other learners, the child with a learning difficulty tends to feel freer to ask an adult (teacher) for explanations without the fear of appearing “stupid” – as is the case for most children.
A supporting teacher can be identified to render support within a more relaxed after-school environment, given the necessary skills needed. Such a teacher is likely one who has shown concern about the child even before the assessment; this may or may not be the regular class teacher. Other sources of support may include student trainee teachers in institutions of higher education (under the supervision of their lecturers), who can benefit from applying their theoretical knowledge while helping learners with learning difficulties.
Table 26. Objects of support
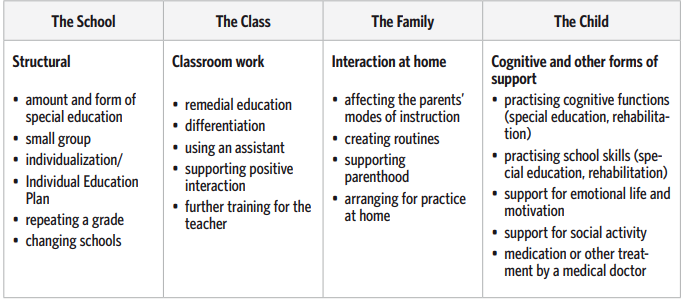
Direct teaching and teaching strategies often achieve better results in school learning than forms of remediation, which focus only on background cognitive functions (such as perception processes) that are difficult to conceptualise. Children with difficulties in perception functions benefit from teaching strategies. Children with normal learning skills create good learning strategies naturally as they grow older and as they are being taught. Among children with learning difficulties, learning strategies may remain ineffective or they may have difficulties in finding independently appropriate strategies for each situation. Children struggling with learning disabilities are often passive in regard to their own learning.
In addition to supporting the child directly, it is important to also think of ways to support the family. Family support may include supporting the family’s resources, parenting, and/or more directly, how to cope with their child afflicted by the learning disability. Discussions regarding the assessment process create a natural opportunity to support the parents in their child’s upbringing and parenting. An essential part of assessment and discussions is the feedback on the assessment and sharing knowledge about learning disabilities. When the child and their family are first confronted with learning disabilities, they are still unaware of the nature of the learning disability that the child may have. Listening to and educating the family are a significant part of feedback. Parents can also be told of forms of instruction, and methods and routines to make daily life easier. When a child has learning disabilities, homework often causes disproportionate strain and worry for the whole family. Routines and practices can apply particularly to homework, time management solutions, or learner routines (e.g., schedules). If necessary, the family could be referred for longer-term support. Sometimes it may be necessary to create forms of cooperation between the school and the home. Mutual patterns of activities and goals, as well as information which flows between the school and the home, reduce possible conflicts. When setting and monitoring the achievement of objectives is open and mutual, an environment that facilitates learning can be created for the child. This is especially important in the African context, where the role of the family as a stakeholder is not always acknowledged by schools. Teachers and schools should empower parents by recognising the role that the parents can play in giving support at home, which can complement the work done at school. Parents need to be made aware that their children may need to stay after school for extra learning support and may not always be available for the mandatory household chores required of most children.
A child struggling with learning disabilities has usually received remedial and special education, and for many it has been a sufficient help. However, when a child is referred for assessment, additional information is normally required to direct teaching and pedagogical solutions. The cognitive difficulties related to learning disabilities delay learning, but never stop it completely. In a certain sense, learning disabilities are pedagogical challenges and can often be treated with pedagogical methods, i.e., effective teaching. At school, the procedures are mainly focused on teaching, its focus, methods, and supplies. In addition, the focus, methods, and time management of remedial and special education must be reconsidered. Assessing the content and objectives of teaching sheds light on the extent to which the teaching meets the child’s needs. Based on the assessment, teaching is adjusted and made more suitable for the true skills and knowledge of the child. In practice, this often means individualising teaching and making an individual educational plan. Another challenge in the African context is that class sizes are huge whilst resources and support services are limited, as a result of which individual education plans (IEP) may be difficult to implement, but not impossible, if using alternative support methods.
Solutions may also be structural, such as when placing the child in special education in a smaller group, or having him or her repeat a grade. Structural decisions may also result in smallerscale solutions. For example, the headmaster may rule that students who struggle with reading comprehension are allowed to underline text in their schoolbooks, or that teachers with many special education students are offered relevant training.
The general situation of the child’s life may be unfavourable for learning, which may reduce the effect of pedagogical or remedial measures. However, other remedial measures must be determined by assessing how significant the unfavourable psychosocial factors are for learning and the child’s well-being. Sometimes it is necessary, even in connection with learning disability assessment, to treat the child primarily with other than learning-oriented arrangements, for example, with psychiatric care. In other cases, the family can be helped with counselling or through support discussions with the parents. In some cases, the assessor must try to influence the teacher’s operation by offering him or her additional information or new ways of dealing with problems. In the African context, lack of funding prohibits the implementation of sufficient structural support for students with learning disabilities. For example, placing students in special education environments may not be possible for all students who need it, such as due to lack of space at these facilities. For instance, currently in Namibia, students are only allowed to repeat a grade once within a phase (e.g., once in lower primary phase) and then automatic promotion kicks in, without further individualised assistance necessarily being offered. As textbooks in government schools are the property of the schools, students may not underline text in books, as these need to be used by others the following year.
In practice, planning support is a cooperative effort by the psychologist, the child, the parents, and the teachers. The support plan can be devised simultaneously with the individualisation plan for teaching the child, or in connection with making or updating the child’s individual education plan. On the following page, there is a concrete example of how a child’s support can be planned (Table 27).
The child can be supported in many ways at school. The primary form of support is, naturally, to help the child understand the nature of his or her difficulties and to strengthen his or her feeling that he/she does not have to deal with the difficulty alone. The child must feel accepted. Words are not always enough to reinforce this understanding, and the child needs repetitive, concrete expressions of success and acceptance in several situations. It is also important to create a culture of discussion that emphasises success and future goals. This strengthens the child’s trust that everyone present has the child’s best interest in mind and wants to help him or her. The assessor must concentrate on realistic objectives and arrange a meeting for the relevant stakeholders to determine whether the goals are progressing or have been reached with the agreed methods. This ensures that the child, family, or teachers are not left to cope alone after the assessment, and that the process continues even if help for the difficulties is not immediately found.
On the practical level, the first form of support is adjusting the form and methods of classroom teaching to suit the child’s strengths and weaknesses (in balance with the rest of the class), so that he or she (as well as the other children in the class) can benefit as much as possible from the teaching. The psychologist’s and special education teacher’s task is to support the regular teacher and the possible assistant teacher in their work. At this point, it is also possible to consider the emphases of teaching, the manner in which an assistant could complement the efforts of the teacher, and possibly attending the special education teacher’s small group that has been formed as part of the intervention, without necessarily focusing only on the individual child.
Another significant form of support is remedial instruction given by the class- or subject teacher, the planning of which can also be supported by specialists. Finnish law, for instance, demands that remedial instruction be given to students who temporarily fall behind in their studies or otherwise need special support. The student’s teacher verifies the need for remedial instruction, but the formal decision on the matter is made by the authority or institution empowered with the relevant decision-making, according to the regulations. The student’s guardian must be informed of all remedial instruction, which is most often arranged outside of classes and is not subject to the statutory maximum school hours. Although Namibian law directs that students who fall behind in their learning are to receive learning support, this service is hampered by the inadequacy of human and material resources. Where this service is implemented, it may not always be monitored and evaluated adequately.
Table 27. The support plan for Peter
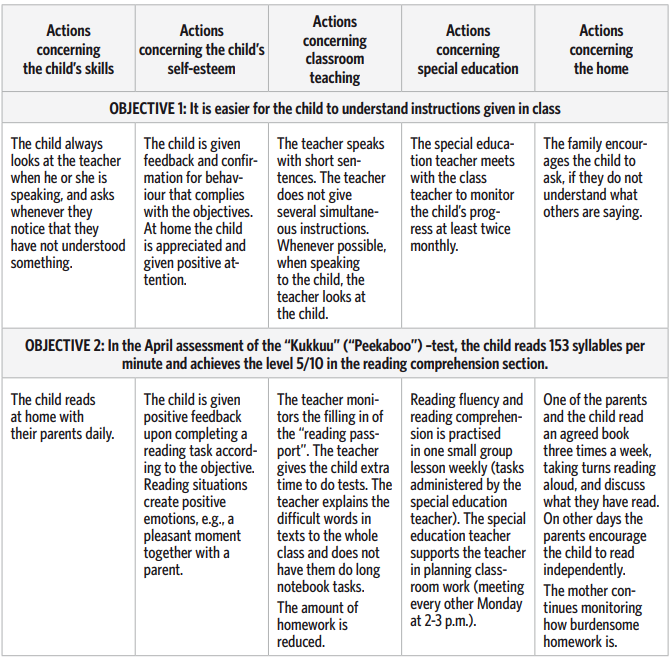
The third form of support is individual or small group special education. Most children with learning disabilities have already received special education before the psychologist’s assessment. However, following the learning disability assessment, there is reason to review the objectives, extent, content and methods of special education. Another question to consider is how to correlate the goals of the work done by the class teacher, possible other teachers, assistants and parents, and how to distribute the work appropriately among the professionals. It is often a major challenge to figure out which objectives are realistic and to find ways of achieving them in addition to the means already tried.
According to Finnish law, a student has the right to receive special education in connection with other teaching if they have learning or adaptation difficulties. The teaching administration decides the extent and manner in which special education is arranged. It can be arranged either outside lessons or as synchronised teaching within the general teaching group. Guardians must be heard before a decision on this is made, and they must be informed of lesson times beforehand. In the African context, intervention is often mainly the responsibility of the class teacher, with some support from parents. The child can also be transferred to special education. This can be done if the child cannot be effectively taught due to a disability, illness, delayed development, emotional disorder, or another similar reason. The transfer can be arranged selectively for one or several subjects.
A formal decision of transferring a student to special education must always be made either at the onset of his/her education or at a later stage. Negotiations must be held with the student’s parents/guardian before the transfer decision. Whenever possible, a psychological or medical examination, or a social report, must also be acquired of the student concerning his or her learning capacity. The teacher and the child’s therapist can also write their own statements. The transfer decision must include the grounds for the transfer. It must also reveal if the general education curriculum or an individualised curriculum will be used for all or only some subjects. As the student makes progress and improves, the transfer decision regarding special education can be cancelled. In extreme cases in Namibia, for example, where children with severe learning difficulties are identified by regional school counsellors and/or psychologists, an affected child may be transferred from the regular school to a special school for students with learning disabilities. These schools offer a stream for both special and regular education. Should a child show enough progress to warrant his or her re-entry into the regular education system, then he or she is transferred back to the mainstream educational system.
An individual educational plan must be made for every student transferred to special education. According to the Finnish National Board of Education (2005), the individual education planmust include:
• A description of the student’s learning abilities, strengths, and special educational needs, and the development of the teaching and learning environment that these needs demand,
• Long- and short-term objectives of teaching and learning,
• Weekly hours per year of the subjects in the student’s curriculum,
• A list of the subjects in which the student’s studies differ from the hours of the curriculum,
• The objectives and central content of the subjects in which the student has an individualised curriculum,
• The principles of the monitoring and assessment of the student’s progress,
• The interpretation and assistant services, other teaching and student welfare services, communication methods, and special support instruments and educational material that participating in teaching requires,
• A description of how the student’s teaching is arranged in connection with other teaching and/or in a special education group,
• The names of the participants involved in arranging the student’s teaching and support services, and their areas of responsibility, and
• The monitoring of the implementation of the support services.
It is also possible to refer a child or adolescent to support services outside the school. In regard to learning disabilities, this usually means ergo- or speech therapy, or (neuro)psychological intervention. Such a form of support can be considered, when:
- Other special forms of support are necessary in addition to the school’s special education,
- The child or adolescent receives special education at school, but due to limited resources, the amount and methods of the school’s special education are not sufficient on their own,
- The child or adolescent is willing and has the energy to participate in therapy or remediation,
- The family is willing to commit themselves to the therapy or remediation, and
- Participation in therapy or remediation does not cause practical complications that are too extensive for the family.
In Namibia, the Ministry of Education has formulated a learning support guide in the form of a Learning Support Teachers’ Manual and a Learning Support Resource Book. These tools are designed so that teachers can offer support to the students in the mainstream class. According to these tools, Learning Support involves planned special support, such as through teaching methods and materials that enable students with learning difficulties and other disadvantaged students to reach essential basic competencies in the different subjects and skills’ (Learning Support Teachers’ Manual, 2010).
Box 6. Description of assessment and intervention clinics and practices in Kenya
There are 73 formalized Educational assessment centers known as Educational Assessment and Resource Center Services (EARCS) in Kenya, 71 of which are the original centers that were formed in each District. Over time the districts have increased and so have the centers. The other 2 of these centers are the Kenya Institute of special Education (KISE) and Kenyatta National Hospital (KNH) educational assessment centers which are the national referral centers. In addition to the 73 assessment centers there are provincial assessment centers in each province which are referred to as Provincial workshops acting mainly as technical support centers and not educational assessment centers. Although these centers were established over 25 years ago, their capacity is not sufficient to handle the assessment and intervention of the children with Learning Disabilities. Majority of the children who come to the EARCS are referred from the various schools around the specific EARCS. A small percentage of children is referred directly from their homes through word of mouth from knowledgeable people in the community. It is evident however that sensitization of special education teachers on Learners with LDs has not been realized and therefore majority of these children are still ignored and eventually forgotten. In the rural remote areas especially, there should be continuous capacity building and sensitization of the special needs teachers so that they are conscious of the challenges and the needs of children with LDs and so that they are aware of assessment centers where they can refer these children for further assessment and intervention. The recently established child development center for children with special needs and disabilities at Getrudes hospital is a good example of the multidisciplinary private clinics available in Kenya.
The Kenyatta University Neuropsychological Assessment and Research Clinic functions to provide quality assessment and remediation, and engages in world-class training and research with a view to satisfying the needs and aspirations of Kenyan children with learning disabilities. In order to address the scope of this mission, the clinic has short- and long-term objectives for guidance. The short-term objectives of the clinics are: to initiate a Neuropsychological Assessment and Research Centre within the Educational Psychology department; to embark on research investigating the prevalence in learning difficulties in Kenya; to start the clinic’s own outreach initiative; to provide advisory services to schools, NGOs, government departments, national assessment centres, etc.; to provide In-service training; and to provide referral services. The long-term objectives are to provide: paediatric counseling, play-therapy, academic training, material development, expert referral services, and capacity building.
Closing Remarks
In this book, we have presented a model by which the personnel of schools, as well as social welfare and health care institutions can perform learning disability assessment. The foundational principle of the model is a comprehensive approach that respects the family and the child. In the model, the child’s situation is looked at broadly by examining the phenotypical problem, the child’s development, test data, and intervening (modifying) factors. When data has been gathered from these four areas, it is possible to view the child as an individual and the child’s family as a unique unit. This respects the fact that both every child and family have their own history and unique story.
The focal points in our book have been the child, the family, the school and the tools of assessment. The professionals themselves (teachers, speech therapists, therapists, or psychologists) have not been examined. They also have their own history, experiences and life circumstances which affect interaction and that are inevitably reflected in their work. Each child and family produces unique emotions and experiences, which the professional interprets according to his or her own experience and history, both consciously and subconsciously. During the assessment process, the professional has to assume various roles, some of which feel natural and comfortable, and some that may feel unpleasant. Not only is the professional one of the parties in the interaction, but he or she also has power and responsibility because of his/her position. How professionals define their own role and overcome the challenges confronting their own emotions largely determines how well they feel they are succeeding in their work. The fact that these issues have not been dealt with in this book does not mean that we think they are insignificant. On the contrary – in our experience, the professional’s role and the emotions stirred up by the children and families all influence the basic conditions of the environment in which learning, teaching, and development take place We felt that this area deserves its own book. Last but not least, we wish to emphasise the use of common sense and practical solutions in developing the provision of a school career to children with learning disabilities that is as smooth as can be. With this in mind, it should be easy to use and apply the specific information and methods that this book provides. Ultimately, the most essential issues in our approach are interaction between the stakeholders and the mutual search for meaningful solutions to the needs of students with learning difficulties and disabilities. If cooperation can be fostered during the assessment process, and all parties are committed to working towards the same objective, it is already a considerable step forward in improving the child’s situation.
References
Goldstein, S. &. Reynolds C.R. (1999) (Eds.). Handbook of Neurodevelopmental and Genetic
Disorders in Children. New York: The Guilford Press.
Kemp S. L., Kirk, U. & Korkman, M. (2001). Essentials of NEPSY Assessment. New York: John Wiley & Sons, Inc.
Kolb, B., & Whishaw, I. Q. (2003). Human Neuropsychology (5th edition). New York: Worth Publishers.
Luria, A.R. (1973). The working brain. London: Penguin Books. Ministry of Education. (2010). Learning Support Resource Book. Okahandja: Namibia Institute of Educational Development.
Puente, A.E. & McCaffrey, R.J. (1992) (Eds.). Handbook of Neuropsychological Assessment: A Biopsychosocial Perspective. New York: Plenum Press.
Sattler, J.M. (2001). Assessment of Children. Cognitive Applications (4th edition). San Diego: Jerome M. Sattler Publisher, Inc.
Yeates K.O., Ris, M.D. & Taylor H.G. (2000) (Eds.). Pediatric Neuropsychology. Research, Theory, and Practice. New York: The Guilford Press.

Further information
Learning disabilities and developmental disorders – African perspective
Abosi, O, (2007). Educating children with learning disabilities in Africa. Learning Disabilities Research & Practice, 22, 3, 196–201.
Cole, M. (2005). Cross–cultural and historical perspectives on the developmental consequences of education. Human Development, 48, 195–216.
Engle, P.L., Black, M.M., Behrman, J.R., de Mello, M.C., Gertler, P.J., Kapiriri, L., Martorell, R., Young, M.E.. and the international Child Development Steering Group (2007). Child development in developing countries 3. Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet, 369, January 20, 229–242.
Graham-McGregor,S., Cheung, Y.B., Cueto, S., Glewwe, P.,Richter, L.,Strupp, B. and the international Child Development Steering Group (2007). Child development in developing countries 1. Developmental potential in the first 5 years for children in developing countries. Lancet, 369, January 6, 60–70.
Grigorenko, E.A., Jarvin, L., Kaani, B., Kapungulya, P.P., Kwiatkowski, J. & Sternberg, R.J.
(2007). Risk factors and resilience in the developing world: one of many lesions to learn.
Development and Psychopathology, 19, 747–765.
Mpofu, E., Peltzer, K., Shumba, A., Serpell, R., & Mogaji, A. (2005). School psychology
in sub-Saharan Africa: results and implications of a six-country survey. In C.L. Frisby &
C.R.Reynolds (eds.) Multicultural school psychology. (1128–1150). Hoboken NJ: John Wiley
& Sons.
Ngorosho, D. (2011). Literacy skills of Kiswahili speaking children in rural Tanzania. The role of home environment. Åbo Akademi University, Vasa. Comprehensive summary online: https:/www.doria.fi/handle/10024/67004
Nyirenda, T. (2011). A miracle life. Bloomington: AuthorHouse.
Serpell, R. (1993). The significance of schooling. Life-journeys in an African society. Cambridge: Cambridge University Press.
Walker, S.P., Wachs, T.D., Gardner, J.M., Lazoff, B., Wasserman, G.A. Pollitt, E., Carter, J.A., and the international Child Development Steering Group (2007). Child development in developing countries 2. Child development: risk factors for adverse outcomes in developing countries. Lancet, 369, January 13, 145–157.
Learning disability – general textbooks
Campbell, J.I.D. (Ed.) (2005). Handbook of mathematical cognition. New York: Psychology Press.
Hulme, C. & Snowling, M.J. (Eds.) (2009). Developmental Disorders of Language Learning and Cognition. United Kingdom: Wiley-Blackwell.
Pennington, B. (2009). Diagnosing Learning Disorders, Second Edition: A Neuropsychological Framework. New York: The Guilford Press.
Swanson, H.L., Harris, K.R., & Graham, S. (Eds.) (2003). Handbook of learning disabilities. New York: The Guilford Press.
Assessment
Grigorenko, E.L.(ed.)(2009). Multicultural psychoeducational assessment. New York: Springer Publishing Company.
Kemp, S.L. & Korkman, M. (2010). Essentials of NEPSY II assessment. New York: John Wiley & Sons.
Miller, D.C. (Ed.) (2010). Best Practices in School Neuropsychology. Guidelines for Effective Practice, Assessment, and Evidence-Based Intervention. Hoboken, New Jersey: John Wiley & Sons.
Ketonen, R., & Mulenga, K. (2002). The Basic Skills Assessment Tool for Reading and Writing (BASAT) and The Users’ Guide. ESSP3 Program and the Ministry of Education in Zambia.
Ketonen, R., & Kalima, K. (2003). Intervention Guidelines for Reading and Writing. English and seven Zambian local languages. ESSP3 program and the Ministry of Education in Zambia.
Diagnostic Manuals
American Psychiatric Association (2004). Diagnostic and statistical manual of mental disorders. Fourth edition. DSM-IV. Washington, DC: American Psychiatric Association.
World Health organization (1992). The ICD-10 classification of mental and behavioural disorders. Clinical descriptions and diagnostic guidelines. Geneva: World Health Organization.
World Health organization (1993). The ICD-10 classification of mental and behavioural disorders. Diagnostic criteria for research. Geneva: World Health Organization.
Learning disability interventions
Fletcher, J.M., Lyon, G.R., Fuchs, L.S. & Barnes, M.A. (2007). Learning disabilities. From identification to intervention. New York: The Guilford Press.
Fletcher-Janzen, E., & Reynolds, C.R. (Eds.) (2008). Neuropsychological perspectives on learning disabilities in the era of RTI. Hoboken, New Jersey: Wiley.
Frederickson, N., & Cline, T. (Eds.) (2002). Special educational needs, inclusion and diversity: a textbook. Buckingham: Open University Press.
Mitchell, D. (2008). What really works in special and inclusive education. Using evidence-based teaching strategies. New York: Routledge.

Appendix
Appendix 1. Preliminary support planning form
Appendix 2. Referral to assessment because of learning problems (PART I)
Appendix 3. Questionnaire for the school (PART II)
Appendix 4. Evidenced-based teaching strategies for children with learning disabilities